Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200925_007
| Complex PCI - Bifurcation/Left Main Diseases and Intervention | |
| LM Bifurcation with Cardiogenic Shock | |
| Thanawat Suesat1 | |
| Khon Kaen Hospital, Thailand1, | |
|
[Clinical Information]
- Patient initials or identifier number:
mrs. O N
-Relevant clinical history and physical exam:
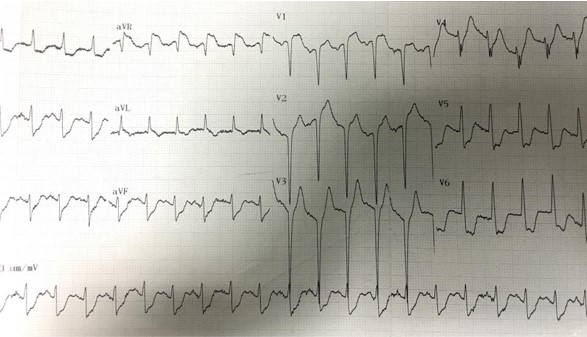
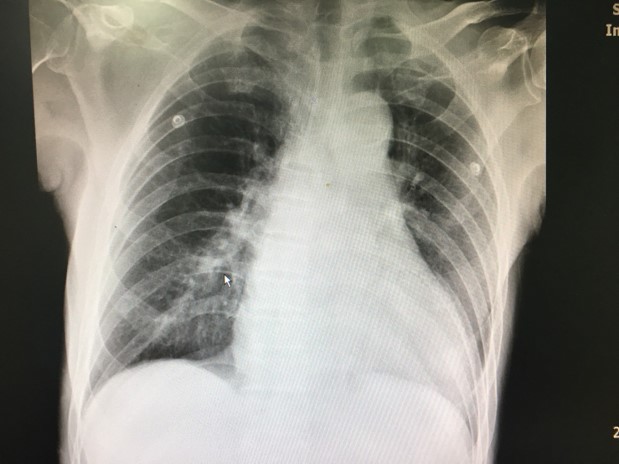
82 year old Thai femaleCC: chest pain for 2 day underlying disease DM , HT , CKD , old CVA , COPDBP : 80/50 mmHg , RR 20 bpm Good consciousness normal heart sound , lung clear , no edema Dx . NSTEMI high risk with cardiogenic shock blood test BUN 60 , Cr = 3.2 , Trop T 556 ECG : Q V1-V3 , ST elevation V1 , AVR and generalized ST depression CXR : mild cardiomegaly Echo : mild LV dilatation , hypokinesia anterior and lateral wall LVEF = 32 % , mild MR , no clot
  -Relevant test results prior to catheterization:
- Relevant catheterization findings:
CAG : LM: 98 % LM stenosis from ostial to distal bifurcation ( medina 1,0,1 )LAD : 50 % mid LAD stenosis LCX : 60 -70 % ostial LCX stenosis , 70 % mid LCX stenosis
RCA : 50 -60 % mid RCA stenosis |
|
|
[Interventional Management]
- Procedural step:
at first on IABP for hemodynamic support admit @ CCU and patient was advice for CABG , however denied for Sx later developed VT and sent to PCI to LM bifurcationfemoral approach , 7F guiding JL4/side hole to LCAwhisper wire to LAD --> VT then dilated LM with 2.0 x 20 balloon after that wire to LCX and dilated with 2.0 x 20 @ 14 atm --> plaque shift to LAD thenfirst kissing balloon with 3.0 x 20 @ LAD and 2.0 x 20 @ LCX then IVUS was checked show diffused disease from ostial LM-proximal LCX and minimal disease at ostial LADthen DK crush was performed with Xience Prime DES 4.0 x23 @ LAD-LM and Xience Prime DES 3.5 x 23 @ LCX then FKB and final POT IVUS was check for stent optimization and area , FFR mid LCX = 0.85 patient was sent to CCU with stable , off IABP at day 2
patient discharge at day 5 Echo follow up at 3 month LVEF improve to 52 % , FC 2follow up angiogram at 1 year with patent stents , No ISR 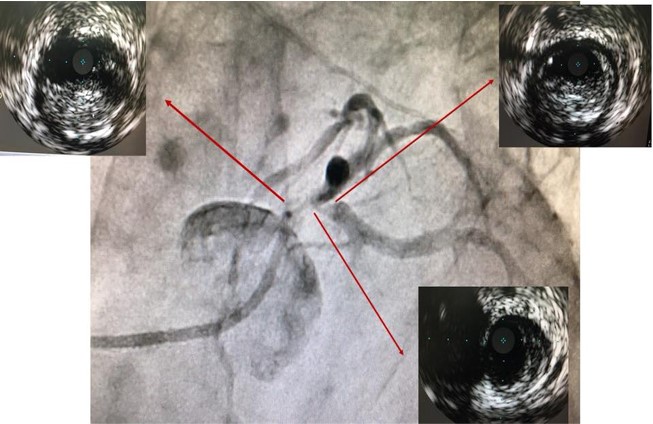 - Case Summary:
LM bifurcation mostly diffused disease and angiography may be inaccurate for assessing disease of ostial both branch IVUS assessment is key for choosing the appropriate LM bifurcation strategy if 2 stent strategy is needed , DK crush provided a reliable with data driven option
|
|