Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200925_006
| Complex PCI - Chronic Total Occlusion | |
| Complex PCI of CTO of LCX Using Provisional Stenting Make It Simple | |
| Islam Elsayed Shehata1 | |
| Zagazig University, Egypt1, | |
|
[Clinical Information]
- Patient initials or identifier number:
A.E.H.
-Relevant clinical history and physical exam:
50Ys old male patient No family history of IHD NSTEMI Hypertensive Not diabetic Dyslipidemic Hemodynamically stable Pulse: 80 bpm BP: 130/80 mmHg LL: No Oedema JVP: Not raised Chest: clear Ht: S1, S2 & 0 Local Exam: free -Relevant test results prior to catheterization:
T-wave inversion in V4, V5 & V6 of ECG wall motion abnormalities in lateral LV wall in TTE. - Relevant catheterization findings:
LCX shows osteal CTO
|
|
|
[Interventional Management]
- Procedural step:
Rt. femoral approach using modified Seldinger technique. Rt. femoral sheath 6F was inserted Lt. and Rt. Judkin catheters used for coronary angiography or Lt. and Rt. coronary arteries. LM: was normal and bifurcates into LAD & LCX. LAD: was atherosclerotic vessel without significant lesions LCX: was totally occluded from its ostium with retrograde filling from Rt. system. RCA: Atherosclerotic vessel without significant lesion Guiding catheter : JL4 Guide wire: BMW universal introduced distally into LCX and LAD. Predilatation balloon: introduced over the guide wire into LCX CTO then multiple inflation by compliant balloon (1.5 X 15 mm) inflated at 14 ATM. Stent: Promus Premiere (3X 20 mm) positioned at ostium of LCX and inflated at 14 ATM with TIMI III flow and no complications. 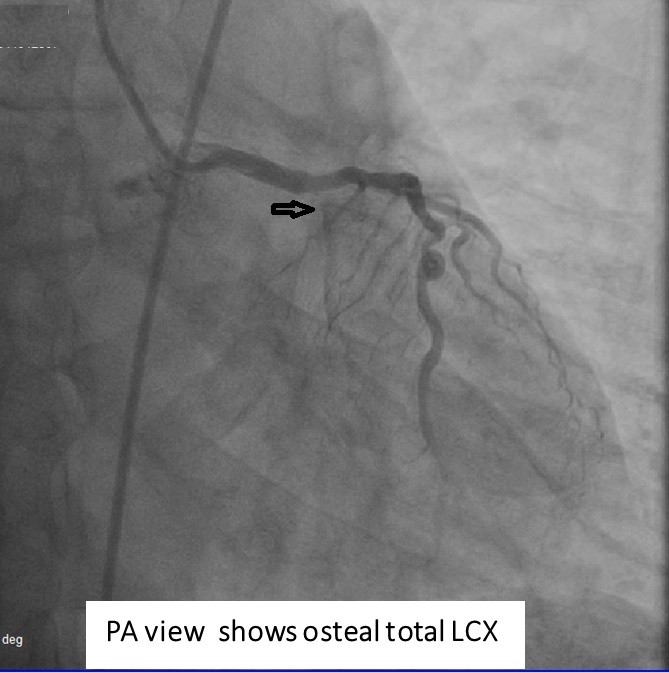 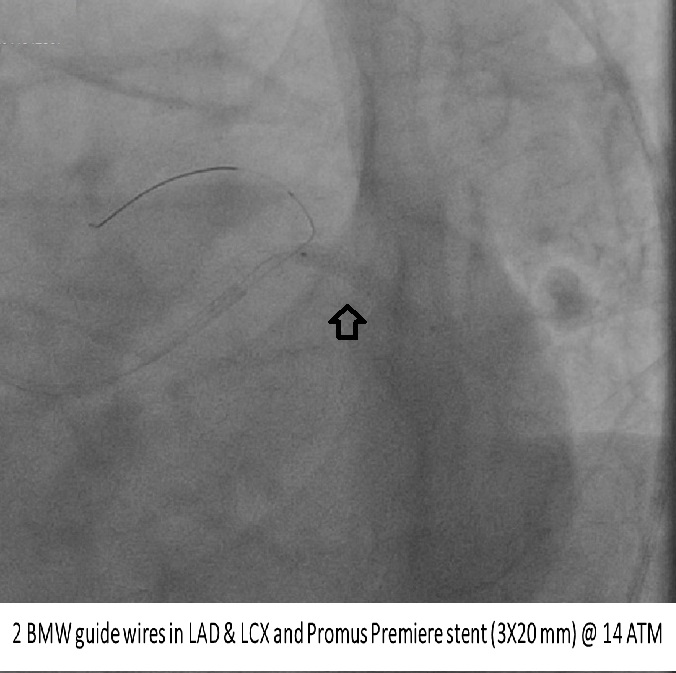 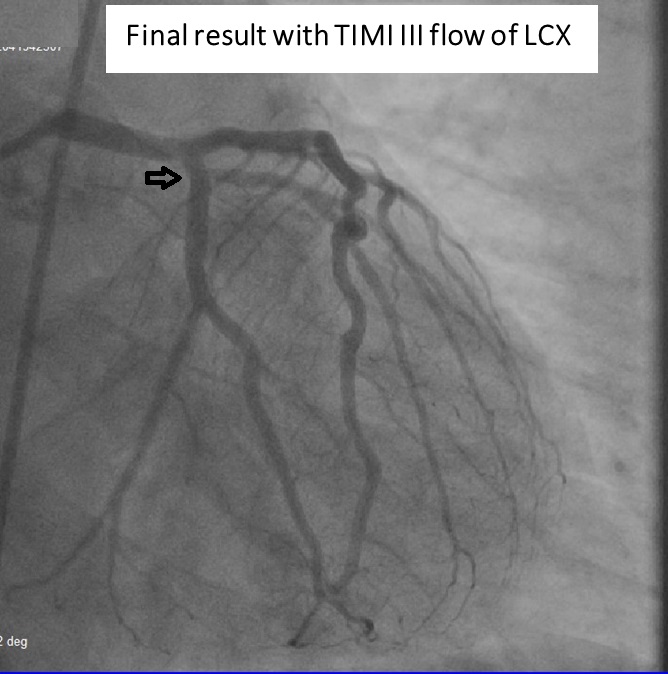 - Case Summary:
Take home message: 1-Simplify your procedure as much as possible for patient safety. 2-Take your time to put your plan before intervention of CTO lesion. 3-Protect your side branch by another wire during intervention with bifurcational lesions. 4-Start by soft wire for CTO lesion then use wire escalation accordingly. 5-Provesional one stent technique can e used in certain cases of osteal LAD or LCX CTO with consideration to anatomical variations. 6-Be ready to change your plan if any complication occurs. |
|