Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200925_003
| Complex PCI - Bifurcation/Left Main Diseases and Intervention | |
| Severe Stenotic Tandem Left Circumflex Lesion Involving Left Main Trunk Treated with Two Different Stenting Techniques | |
| Hironobu Kikuchi1, Tatsuya Kamon1, Kazutoshi Hirose1, Hiroki Shinohara1, Hiroyuki Kiriyama1, Akihito Saito1, Mizuki Miura2, Shun Minatsuki1, Arihiro Kiyosue1, Satoshi Kodera1, Jiro Ando1, Norifumi Takeda1, Issei Komuro1 | |
| The University of Tokyo Hospital, Japan1, University Hospital Zurich, Switzerland2, | |
|
[Clinical Information]
- Patient initials or identifier number:
YK022967038
-Relevant clinical history and physical exam:
 -Relevant test results prior to catheterization:
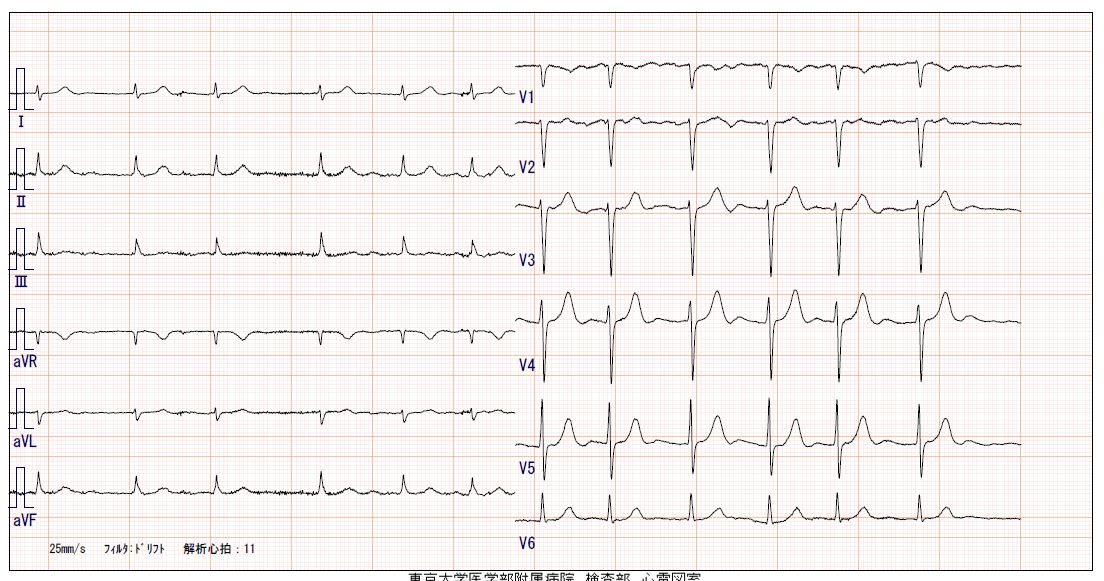
He is relatively fat with body weight of 74.0 kg and body height of 162.7 cm(BMI 28.0). About blood test, he had no anemia, normal renal function of eGFR 65 ml/min/1.73m2. ECG showed atrial fibrillation with heart rate at 76/min with no abnormal ST change. Chest X-ray showed no congestion nor cardiomegaly. Transthoracic echocardiogram showed good left ventricular contraction without asynergy(EF 68%), chamber/wall dimension and valves were almost normal.
  - Relevant catheterization findings:
CAG showed 2VD of LAD proximal lesion and LCxproximal lesion involving high lateral branch(HL) and left main trunk(LMT).Wehad selected elective revascularization by percutaneous coronary intervention(PCI).LAD lesion was treated with drug eluting stent(DES). Then we had staged PCI toresidual LCx stenosis. Target lesion was LCx proximal severe stenotic lesionwith HL arising from the lesion. HL also has stenosis. The lesion seemed to betortuous and severely calcified by CAG. Syntax score I was 25 and AHA lesion classificationwas type C.
|
|
|
[Interventional Management]
- Procedural step:
PCI was performed through left radial access. We engaged guiding catheter(7F Hyperion SPB 3.75; Asahi intecc; Aichi,Japan) and crossed 0.014 inch guidewire(GW) to LAD, LCx and HL. Intravascularultrasound (IVUS) catheter couldn’t pass through neither HL nor LCx. After predilatated the LCx/HL using 2.0/15 mm balloon, IVUS passed and revealed the lesion with severe calcification in both LCx and HL carina. To further dilatate and modificate the lesion, we used scoring balloon(Lacrosse NSE; Nipro: Osaka,Japan) gaining backup force by anchor balloon technique with 3.0 mm balloon in LAD. Lacrosse NSE is a balloon catheter with three nylon elements along the outsideof it. We deployed DES(Ultimaster Tansei 2.5/12 mm; Terumo; Tokyo, Japan) from LCx os to HL. We crossed the GW through jailed strut to LCx, and deployed DES(Ultimaster Tansei 2.5/18 mm; Terumo) from LMT body to LCx. After dilatating LMT proximal(POT technique), we crossed GW to LAD. For not detecting evident plaque nor stenosis in LAD proximal, we decided to treat LMT bifurcation by kissing balloon technique (KBT) though we treated the HL bifurcation by culottestenting technique with 2 balloons(3.0 mm in LMT-LAD and 2.0 mm in LMT-LCx. LMT).Proximal stent edge was postdilatated by 4.5 mm balloon. Final IVUS observation showed no malaposition, nor injury. We got good coronary flow in LAD, HL, andLCx at final angiography, and finished the procedure.
- Case Summary:
We successfully treated tandem LAD/LCx andLCx/HL bifurcation lesion by DESs. Bifurcation lesions are treated by 1stent(stenting with or without KBT, etc.) or 2 stent(crush/culotte technique, etc.) strategies according to and considering the conditions of the lesion(morphology of arteries, extent of calcification, plaque volume, etc.). We should carefully select these stenting techniques which is most appropriate for each case. Here,we report the tandem bifurcation lesion successfully treated using two different stenting techniques(culotte stenting and KBT).
|
|