Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200925_001
| Adjunctive Procedures (thrombectomy, artherectomy, special balloons) - Adjunctive Procedures | |
| Percutaneous Management of Giant Coronary Aneurysm of RCA and Subsequent In-stent Restenosis of Covered Stent | |
| Chirag Sheth1 | |
| Rhythm Heart Institute, India1, | |
|
[Clinical Information]
- Patient initials or identifier number:
RS
-Relevant clinical history and physical exam:
50 years old male underwent PCI with DESto RCA (3.5 x 48 mm) for chronic total occlusion of mid RCA in Sept.2018. Coronary angiogramfor new onset angina in Feb.2019 showed giantcoronary aneurysm from proximal RCA, possibly from proximal edge of the stent. Two overlapping covered stents 4x19 mm & 3.5x19 mm were deployed for treating coronary aneurysm with IVUS/OCT study. For recurrent angina in July2019 , angiography showed proximal&distal edge restenosis of covered stents. -Relevant test results prior to catheterization:
- Relevant catheterization findings:
In Feb 2019: Right coronary artery showed giant coronary aneurysm from proximal RCA, possibly arising from proximal edge of the stent with a broad base. Left coronary artery showed 80% diffuse disease in mid LAD with normal LCx. RCA was treated with covered stents with IVUS/OCT guidance in March 2019. PCI For recurrent angina in July2019 , angiography showed discrete proximal & distal edge restenosis of covered stents in RCA.
|
|
|
[Interventional Management]
- Procedural step:
Transfemoral approach, 7f JR 3.0 guiding catheter. Baseline IVUS study done. Cutting balloon dilatation done with Flextome 3.5x10 mm at 6-8 atm pressure at site of both proximal and distal edge restenosis. NC balloon dilatations were done with 4x12 mm at proximal edge restenosis and 3.5x12 mm at distal edge restenosis at 18-20 atm pressures. Finally 4x44 mm DES was deployed from ostium of RCA at 16 atm pressure. Postdilatation was performed with 4x12 mm balloon at 18 atm pressure. Final IVUS study was performed for guiding optimisation of PCI.
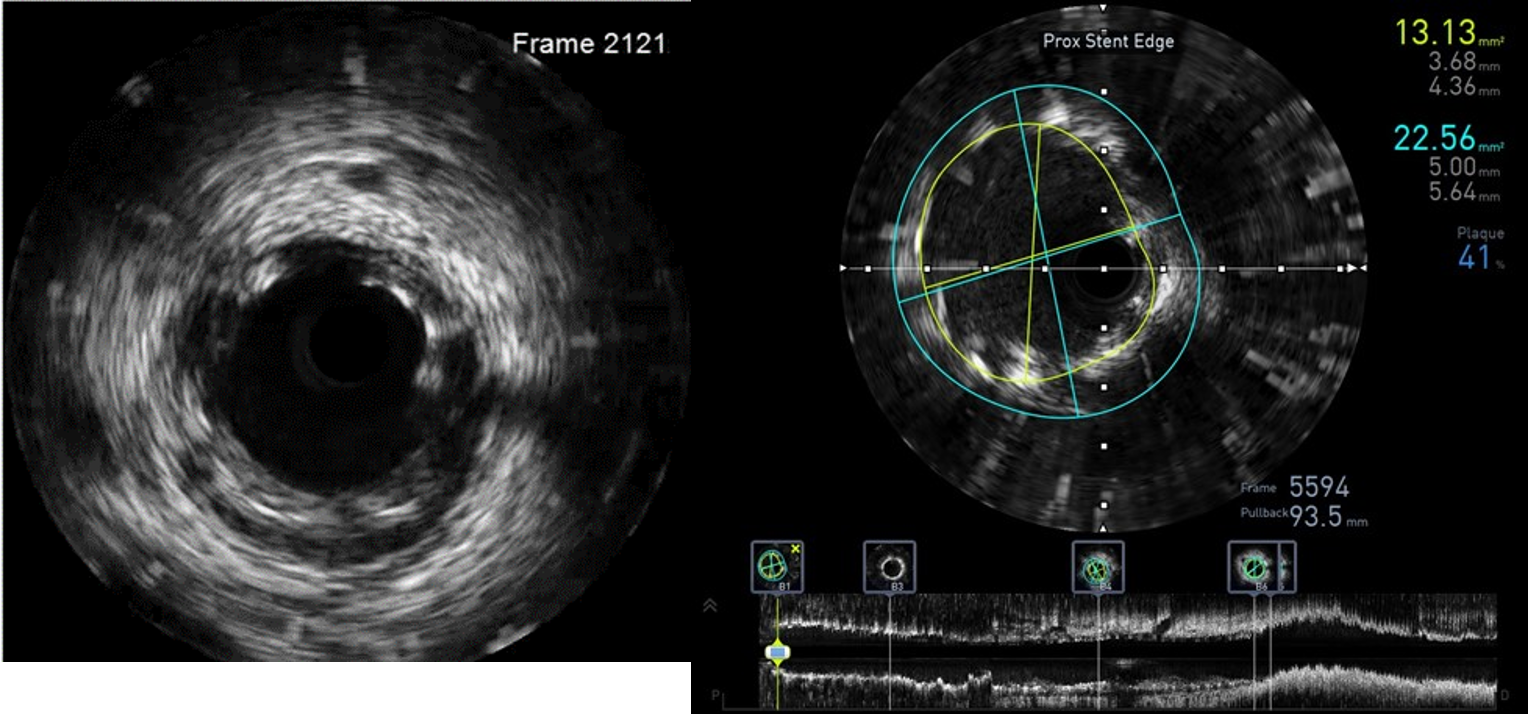 - Case Summary:
Complex interaction of injury to media due to true-false-true passage of guidewires in index PCI for CTO and DES deployment in RCA led to Giant coronary aneurysm. PCI with overlapping covered stent deployment with image guided optimisation is a feasible strategy for treating such large aneurysms. Covered stents have high risk of instent restenosis, which could be treated effectively with Flextome cutting balloon dilatations and then subsequent DES implantation with good clinical 1 year outcome.
|
|