Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200924_011
| High-Risk Intervention (diabetes, heart failure, renal failure, shock, etc) - High-Risk Intervention | |
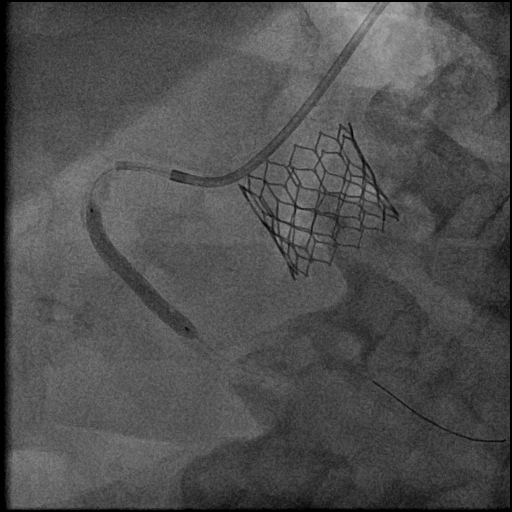
| Optical Coherence Tomography Guided Percutaneous Coronary Intervention Following Transcatheter Aortic Valve Replacement | |
| Tatsuya Kamon1, Mizuki Miura2, Jiro Ando1, Kazutoshi Hirose1, Hiroki Shinohara1, Hiroyuki Kiriyama1, Akihito Saito1, Shun Minatsuki1, Hironobu Kikuchi1, Arihiro Kiyosue1, Satoshi Kodera1, Norifumi Takeda1, Issei Komuro1 | |
| The University of Tokyo Hospital, Japan1, University Hospital Zurich, Switzerland2, | |
|
[Clinical Information]
- Patient initials or identifier number:
T.N
-Relevant clinical history and physical exam:
An 84-year-old man presented with dyspnea NYHA III and was referred to our institution for the treatment of severe aortic stenosis. He had chronic kidney disease, prior stroke, and paroxysmal atrial fibrillation. Coronary angiography showed significant stenosis in right coronary artery. Our strategy was to perform TAVR for severe aortic stenosis and PCI for coronary artery disease with minimum contrast volume. At first, he underwent successful TAVR without worsened kidney function.
-Relevant test results prior to catheterization:
Blood test: Hemoglobine 10.6 g/dl, creatine 2.01 mg/dl, estimate glomerular filtration rate 25.3 ml/min/1.73m2.
- Relevant catheterization findings:
Coronary angiography: diffuse moderate stenosis in LAD, diffuse severe stenosis in LCX, diffuse severe stenosis in RCA mid.
|
|
|
[Interventional Management]
- Procedural step:
Staged PCI to RCA was performed. The system was a left radial artery approach and 6Fr sheaths. A6Fr judkin’s right 4.0 was used to engage the RCA and coronary guidewire was advanced to distal RCA. To enhance backup, an extention catheter was inserted up to the proximal part of the RCA. Coronary artery imaging was performed using optical coherence tomography (OCT) with low-molecular-weight dextran without the use of contrast agents. The stenosis lesion was mainly calcification with partial ulceration, and the calcification was mild in thickness. Pre-dilation with 3.0 mm × 15 mm non-compliant balloon was performed, and OCT was performed again to confirm that calcification dissection was occurring. A 3.5 ×34 mm zotarolimus-eluting stent was deployed into RCA mid lesion and expanded at high pressure with 3.0 mm × 15 mm non-compliant balloon. The final OCT demonstrated good apposition and expansion of the stent. There was no vascular injury. A total of 15 ml of contrast agent use was minimal and the treatment was completed without complications. No contrast nephropathy was noted and the patient was discharged on the second postoperative day.
 - Case Summary:
In this case, the patient underwent PCI with minimal contrast using low-molecular-weight dextran OCT as coronary imaging. The use of an extension catheter provided enhanced back-up and clearer images of OCT. OCT with low molecular weight dextran provides more information on vessel size, lesion length and plaque characteristics, which may lead to a reduction in contrast use.
|
|