Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200924_005
| Complex PCI - Chronic Total Occlusion | |
| One Case of Three Chronic Total Occluded Vessels PCI with ECMO Support | |
| Zhao-Hui Liu1 | |
| The Fifth People's Hospital of Chengdu, China1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Male ,50ys
-Relevant clinical history and physical exam:
Edema of both lower limbs for 3 months. Coronary angiography showed chronic coronary occlusion 10 years ago.
DM,without HTN. Quit smoking. BP 125/80mmHg, Double lung breath tone thickened, double lower lung wet rale. Heart boundary expanded to the left, heart rate 80 beats / min, rhythm, each valve auscultation area did not hear pathological murmur. Diagnosis: 1.Coronary atherosclerotic heart disease, ischemic cardiomyopathy; 2. Type 2 diabetes 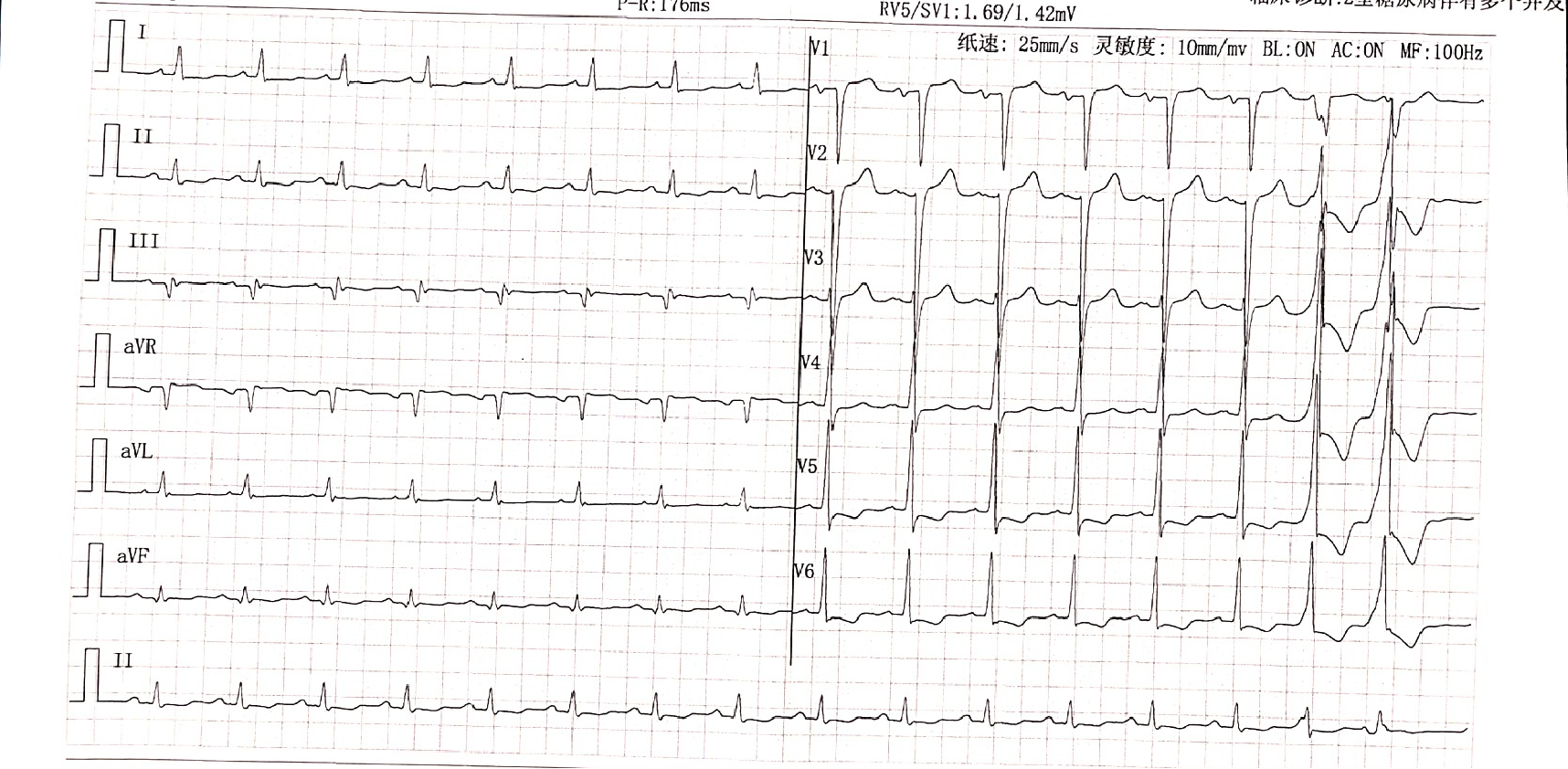 -Relevant test results prior to catheterization:
cTnI (-), BNP (-)
Blood lipids(-) BUN 8.07 mmol/L, sCr 113.1 umol/L↑ UCG LV 64mm,LA 49mm,EF 28% - Relevant catheterization findings:
After cardiac function improvement, CAG. All LAD,LCX and RCA were completely occluded, leaving only intermediate branch.
|
|
|
[Interventional Management]
- Procedural step:
The risk of circulatory collapse during surgery is high. We've done enough risk management:1.ECMO support
2.LM proximal lesions →GC incarceration Assessment LM with IVUS GC do not enter LM The stent is first implanted in intermediate branch to the LM, but affects the IVUS recognition LAD entrance, and the guide wire enters the stump. 2.Handle intermediate branch - LM Balloon :1:3 Dilute contrast agent Rapid release 3.When R-CART, LM had too many instruments Full antigrade preparation:IVUS find stump and confirm guide wire entry ,2.0 mm pre-expand → for R-CART preparation. When antigrade preparation is complete, only guide wire is retained. Retrograde MC only to LAD openings, do not enter LM, reverse rendezvous, or replace RG3 or capture guide wires. After the forward guide wire enters, withdraw the reverse system as soon as possible. With ECMO supporting, we implanted 1 stent in intermediate branch,LAD successfully opened and implanted 2 stents. During the operation, the patient repeatedly and violently vomiting, the occurrence of stress upper gastrointestinal bleeding, but blood pressure, ECG stability. At present, the patient has been discharged from hospital. - Case Summary:
1.ECMO is very helpful in very high-risk patients PCI. 2.Read the view carefully before operation, make strategy, plan, define risk and avoid strategy. 3.Rapid conversion strategy to shorten the operation time. Can I only handle the intermediate branch first, after a period of time to deal with the LAD CTO? |
|