Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200924_003
| DES / BVS - Stents (bare-metal, drug-eluting) | |
| Can Stent Apposition be Confirmed by Conventional Angiography? | |
| Mutlu Vural1, Emirhan Hancıoglu2 | |
| Private clinic, Turkey1, Sbu Bagcılar Training and Research Hospital, Turkey2, | |
|
[Clinical Information]
- Patient initials or identifier number:
MMA
-Relevant clinical history and physical exam:
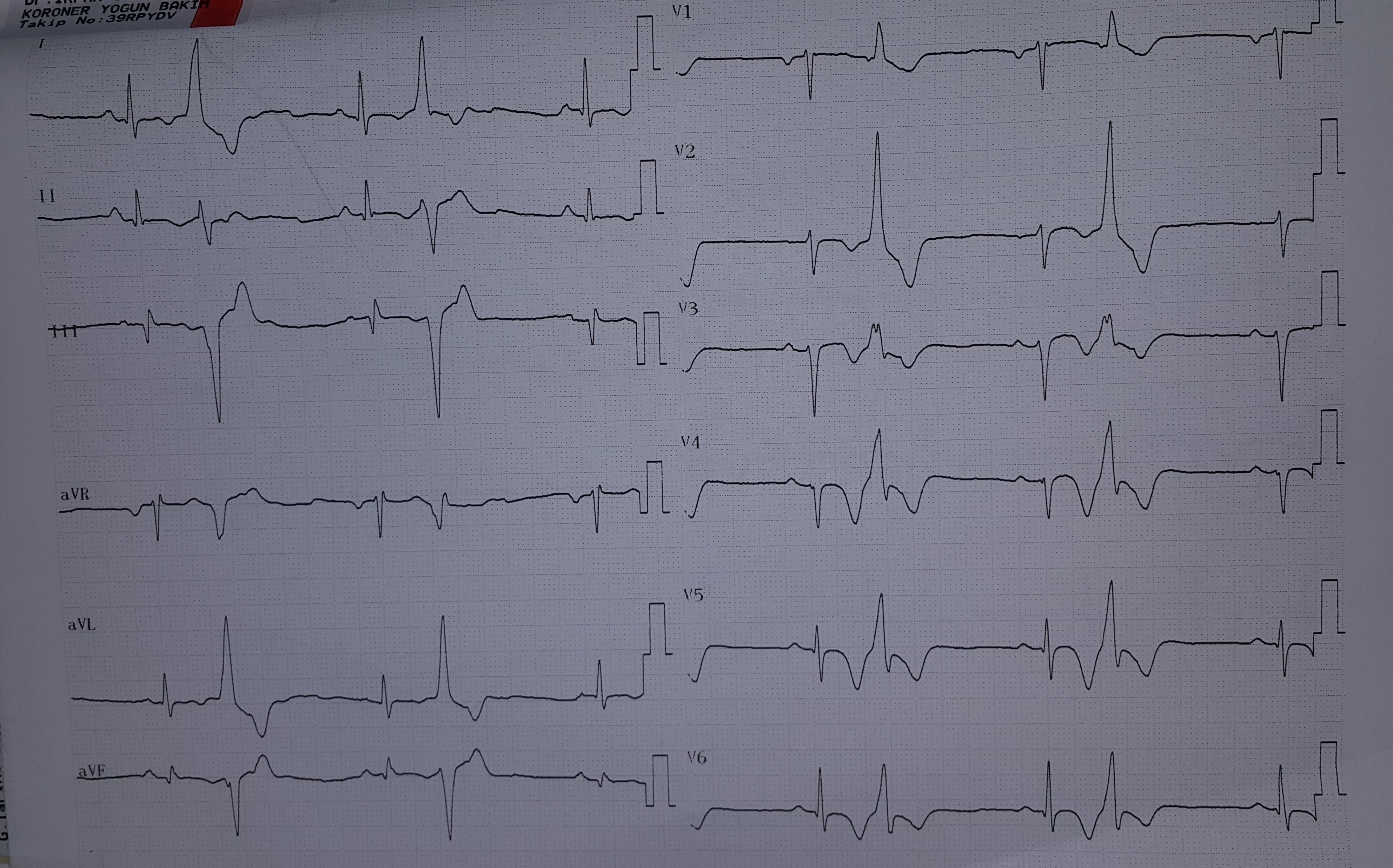
A53 year-old patient without any documented cardiac disease admitted to ouroutpatient clinic with exertional angina pectoris (for 6 weeks) and presyncopeoccured a week ago. He is nondiabetic and ex-smoker. Previous anterior myocardial infarction was shown on electrocardiography (ECG, figure 1). Because he wasstable, an elective coronary angiography has been ordered. Aspirin andbetablocker have been prescribed.
-Relevant test results prior to catheterization:
On ECG, frequent premature ventricular beats and precordial biphasic T-waves have been shown (Figure 1). Biochemical tests were unremarkable. On echocardiography,apical hipokinesia was detected and EF was 0.50.
 - Relevant catheterization findings:
Oncoronary angiography, there was total occlusion of left anterior descendingartery (LAD) at distal portion with retrograde filling with bridge collaterals (video 1). There was slight tapering in the proximal and distal main vessel (before and after side branch). Other coronary arteries were shown to have minimal disease.
 |
|
|
[Interventional Management]
- Procedural step:
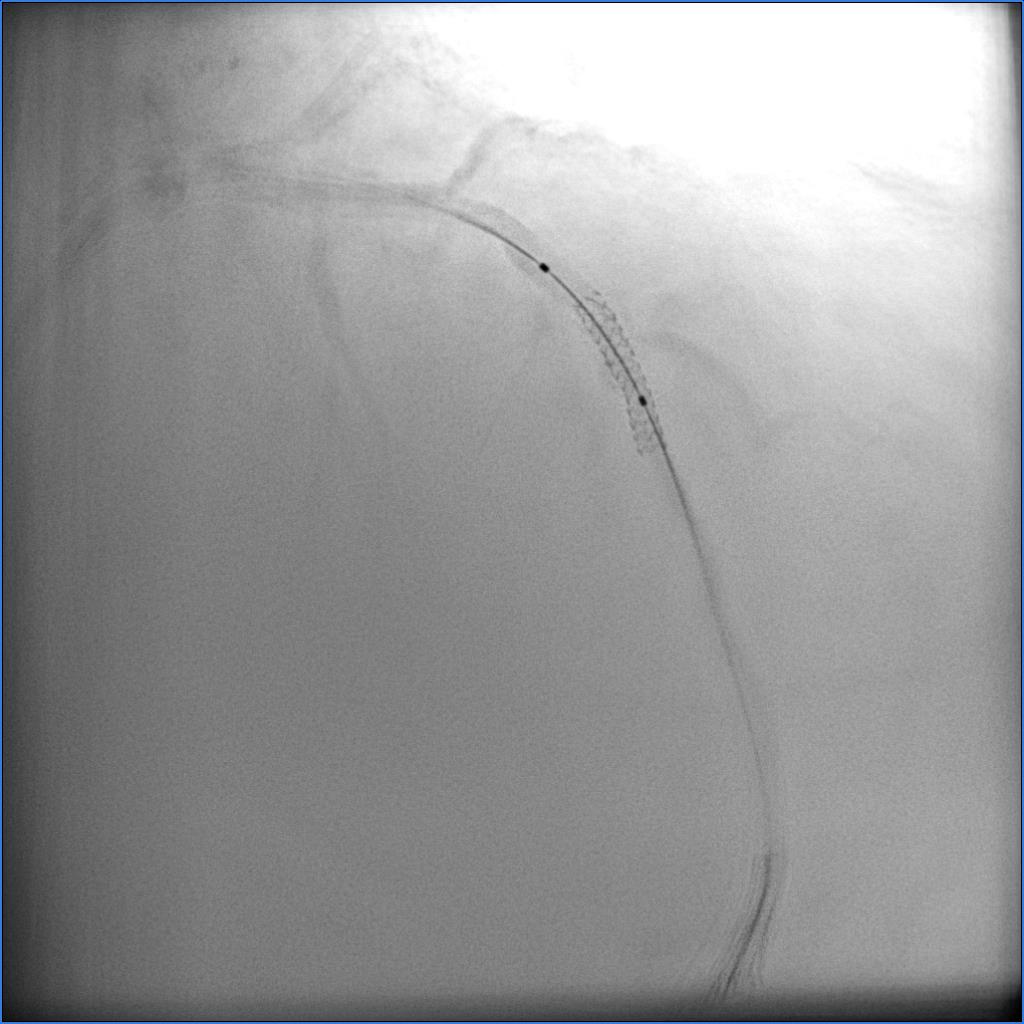
Our plan was provisional stenting in this bifurcation lesion. A 6 Fr EBU 3.75 guide catheter was selected. Wiring with workhorse wire was failed. Then, the lesion has been crossed with a PT-2 after 10 min. work; first to the septal artery then distal LAD. After wire exchange, the lesion was regarded as a balloon undilatable (hardly crossable) lesion ( video 2). So, we suggested that it was a CTO bifurcation (video 3). Then, a 3.0x15 NC balloon was inflated at 18 atm. Later, a 3.0x18 mm DES implanted up to 16 atm. Perfusion to SB was persisted at 14 and 18 atm (video 4 and 5). Then 3.5x10 ballon was inflated for proximal optimisation (POT) at 14 atm. Total SB occlusion (video 6) was used as an indicator for good stent apposition during POT. Because there was TIMI 3 flow in the SB, no further intervention was ordered (video 7).
- Case Summary:
Intracoronaryimaging (IVUS) has vital importance to confirm stent apposition and expansionduring PCIs, but not widely available in the world . Operators should get more information from conventionalangiography to achieve good result in PCI. Injecting a small amount of contrast couldbe a practical way to approve good stent apposition. Side branch(SB) occlusion would be a good marker for optimal stent expansion. Although proximal optimisation especially for proximal main vessel is essential in bifurcation lesions; this technique might decrease unnecessary POTs in some cases, especially proximal and distal main vessel (before and after SB) is not non-tapering.
|
|