Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200923_002
| High-Risk Intervention (diabetes, heart failure, renal failure, shock, etc) - High-Risk Intervention | |
| Primary Angioplasty of Left Main with Cardiogenic Shock & Pulmonary Oedema with IABP Support | |
| Hariom Tyagi1 | |
| Lokpriya Hospital, India1, | |
|
[Clinical Information]
- Patient initials or identifier number:
L K
-Relevant clinical history and physical exam:
This45 year old gentleman- a known case of old AWMI (post PTCA to LAD in 2011)presented to us with severe retrosternal chest pain &dyspnoea a/w sweating for last 3 hours. The patient wasin Killip Class IV with cardiogenic shockand recurrent VT. vECG: LBBB, Diffuse ST depressionin all leads except aVR & V1 & ST elevationin I,aVL & aVR v2 DEcho suggestive of severe LV Systolic Dysfunction( LVEF-20%),SevereMR, Moderate TR ,Moderate PAH -Relevant test results prior to catheterization:
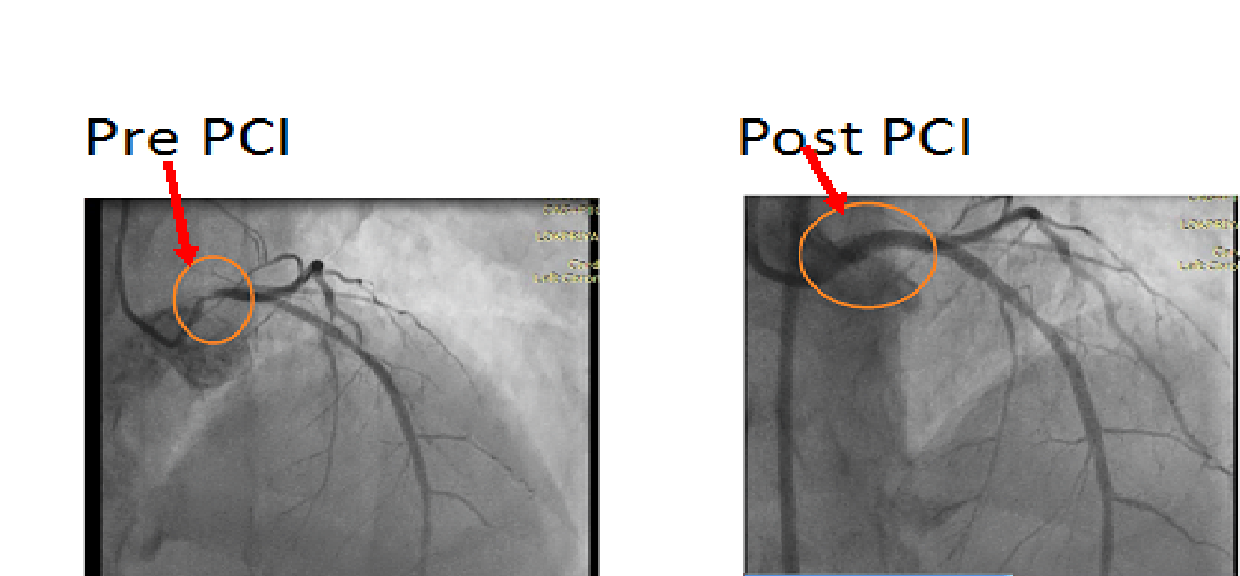
The patient was taken for Urgent CAG withintent to primary angioplasty. Coronary angiography suggested critical LM stenosis with significant ISR of LADstent in proximal part. 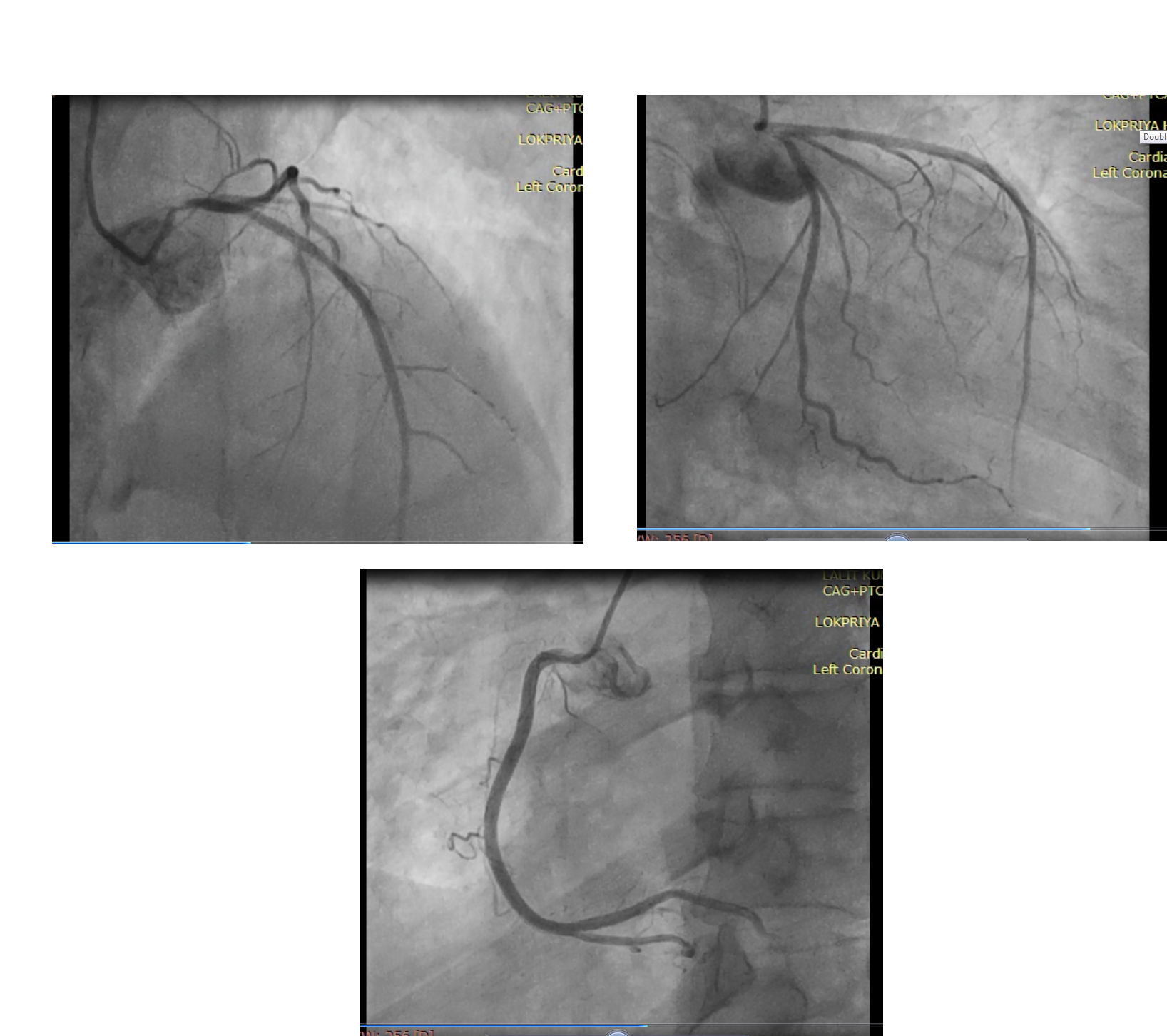 - Relevant catheterization findings:
Patient was put on Intra-aortic balloonpump. JL 3.5- 7F guiding catheter was engaged inleft cusp near LM ostium After crossing the lesion & serial predilatation with semicompliant balloons, 4.0x 23 Xience Prime DES was implanted from LM to LAD covering the ISRsegment. Post dilatation with proximal optimization was done using4.5x 8 mm NC sprinter balloon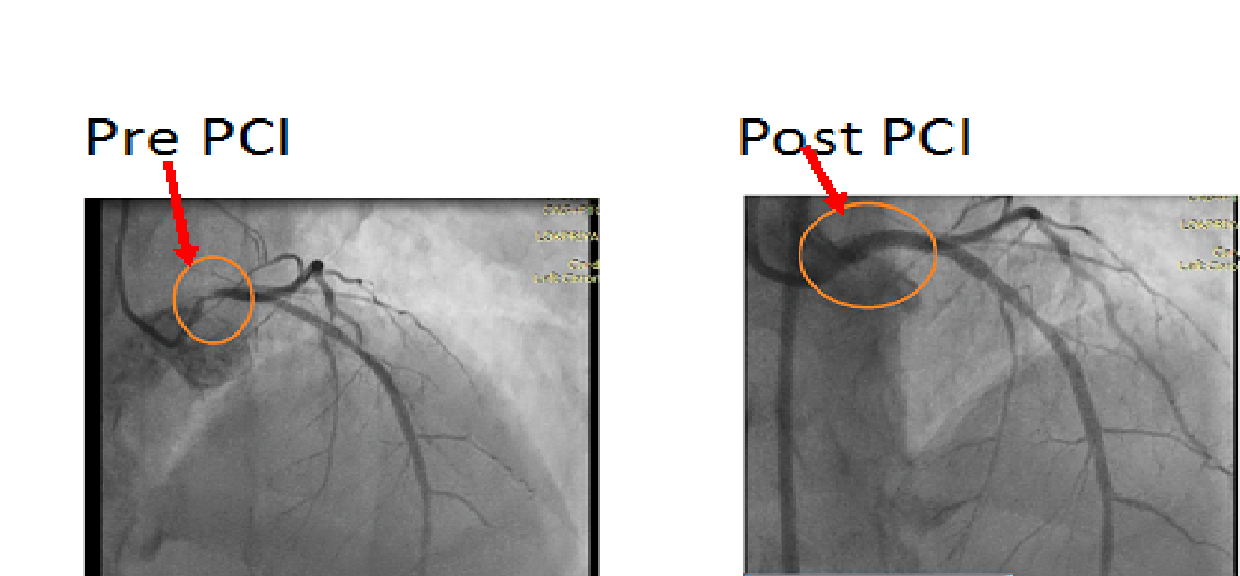 |
|
|
[Interventional Management]
- Procedural step:
After explaining the high risk & takingconsent of death on table IABP support (34cc linear balloon) was put through leftfemoral artery.
 - Case Summary:
Significant (defined as a greater than 50 percentangiographic narrowing) left main coronaryartery disease (LMCAD) is found in 4 to 6 percent ofall patients who undergo coronary arteriography. It is associated with multivessel coronary artery disease about 70 percent of the time
|
|