Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200922_004
| High-Risk Intervention (diabetes, heart failure, renal failure, shock, etc) - High-Risk Intervention | |
| Simplified Left Main Trifurcation PCI in a Patient with High Bleeding Risks | |
| Nay Thu Win1, Hui Beng Koh2, Mohamed Nazrul Mohamed Nazeeb3, Kumara Gurupparan Ganesan3 | |
| Royal Free London, United Kingdom1, National Heart Insitute, Malaysia2, National Heart Institute, Malaysia3, | |
|
[Clinical Information]
- Patient initials or identifier number:
MBLAR
-Relevant clinical history and physical exam:
A 47 years old gentleman, presented with acute pulmonary oedema secondary to non-STEMI at a non-PCI capable center. He was transferred to our center for early coronary angiogram. He has underlying hypertension, type 2 diabetes mellitus and end stage renal failure on regular hemodialysis. He was counselled for coronary angiogram and angioplasty.
-Relevant test results prior to catheterization:
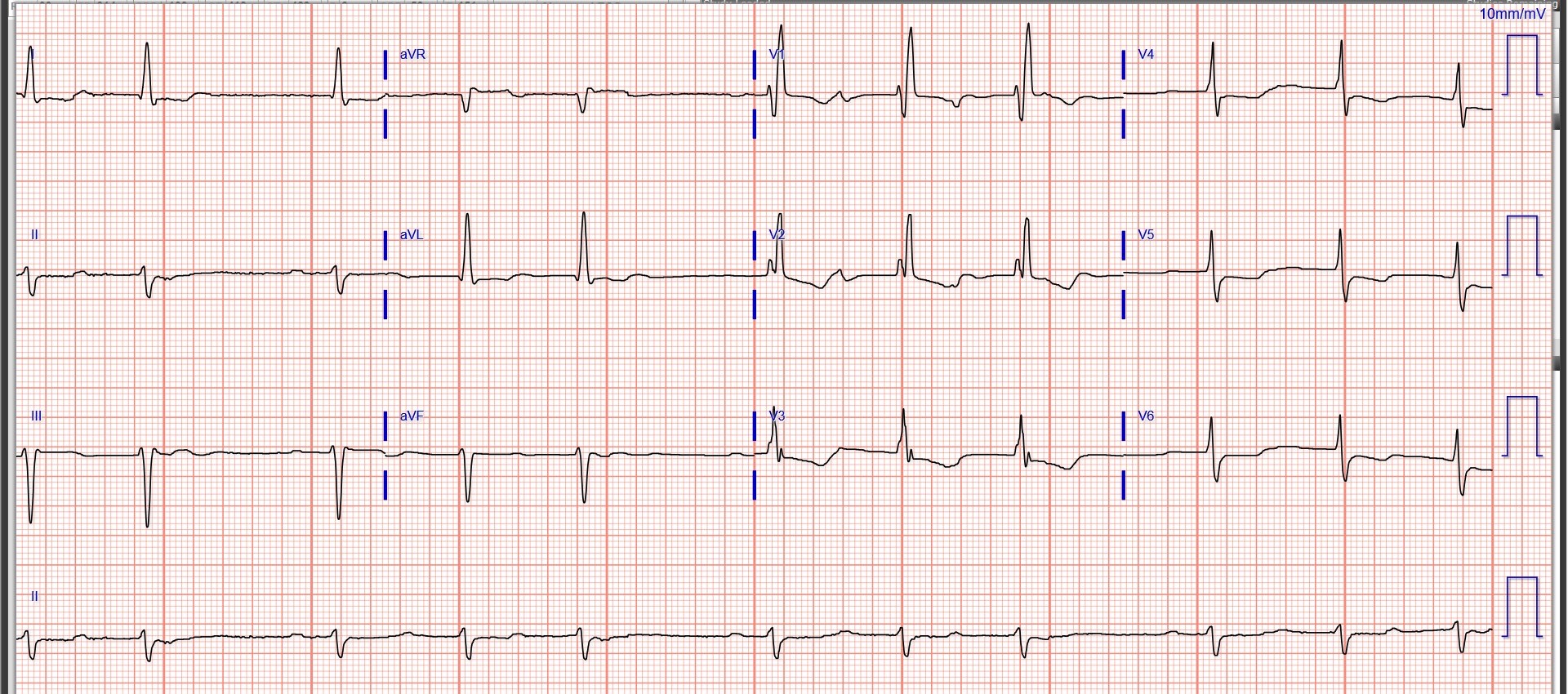
Electrocardiogram showed Prolonged PR interval, Atrial premature complexes, RBBB and LAFB, non-specific STdepression and generalised T inversions. Echocardiogram showed global hypokinesia with left ventricular ejection fraction of 37%. All four chambers are dilated with structurally normal valves. Blood investigations showed hypochromic microcytic anaemia (7.0 g/dl) hence transfused packed cells and optimised iron deficiency anaemia in CKD.
 - Relevant catheterization findings:
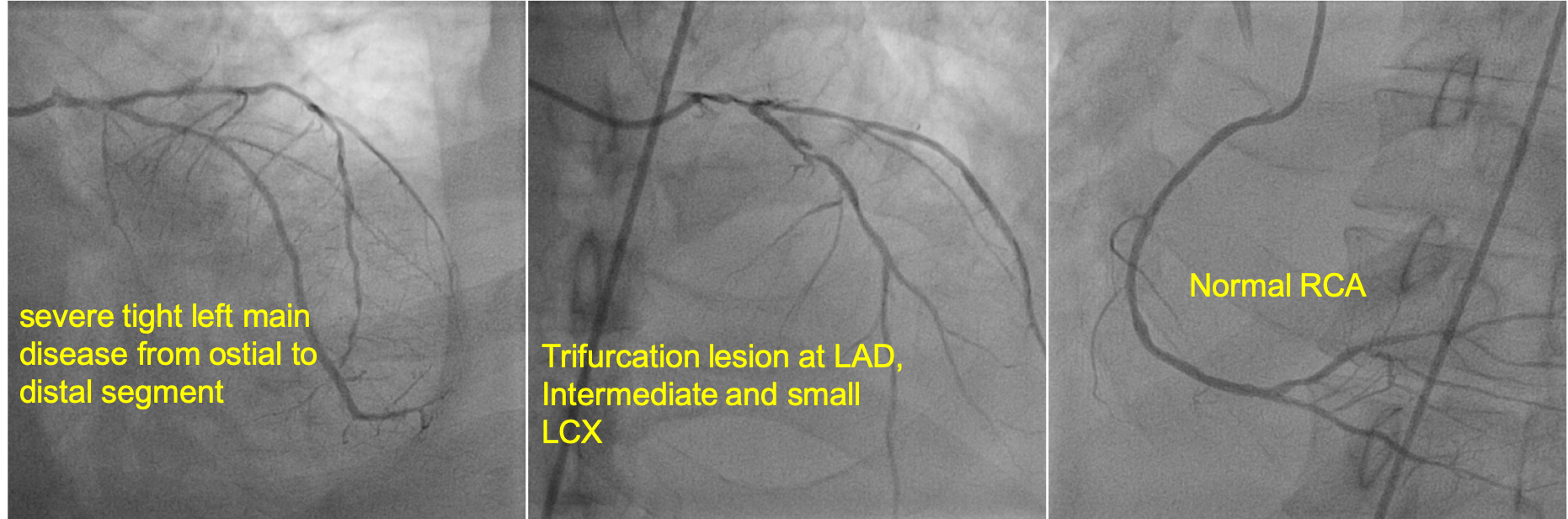
Coronary angiogram revealed severe tight left main from ostial to distal left main, Trifurcation lesion at LAD, Intermediate and LCX with normal right coronary artery. He was counselled for coronary artery bypass graft surgery or high risk PCI for left main trifurcation lesion and explained the high risk of bleeding due to advanced chronic kidney disease and anaemia. After a meticulous discussion, patient opted for high risk PCI. We proceeded complex PCI with provisional stenting approach.
 |
|
|
[Interventional Management]
- Procedural step:
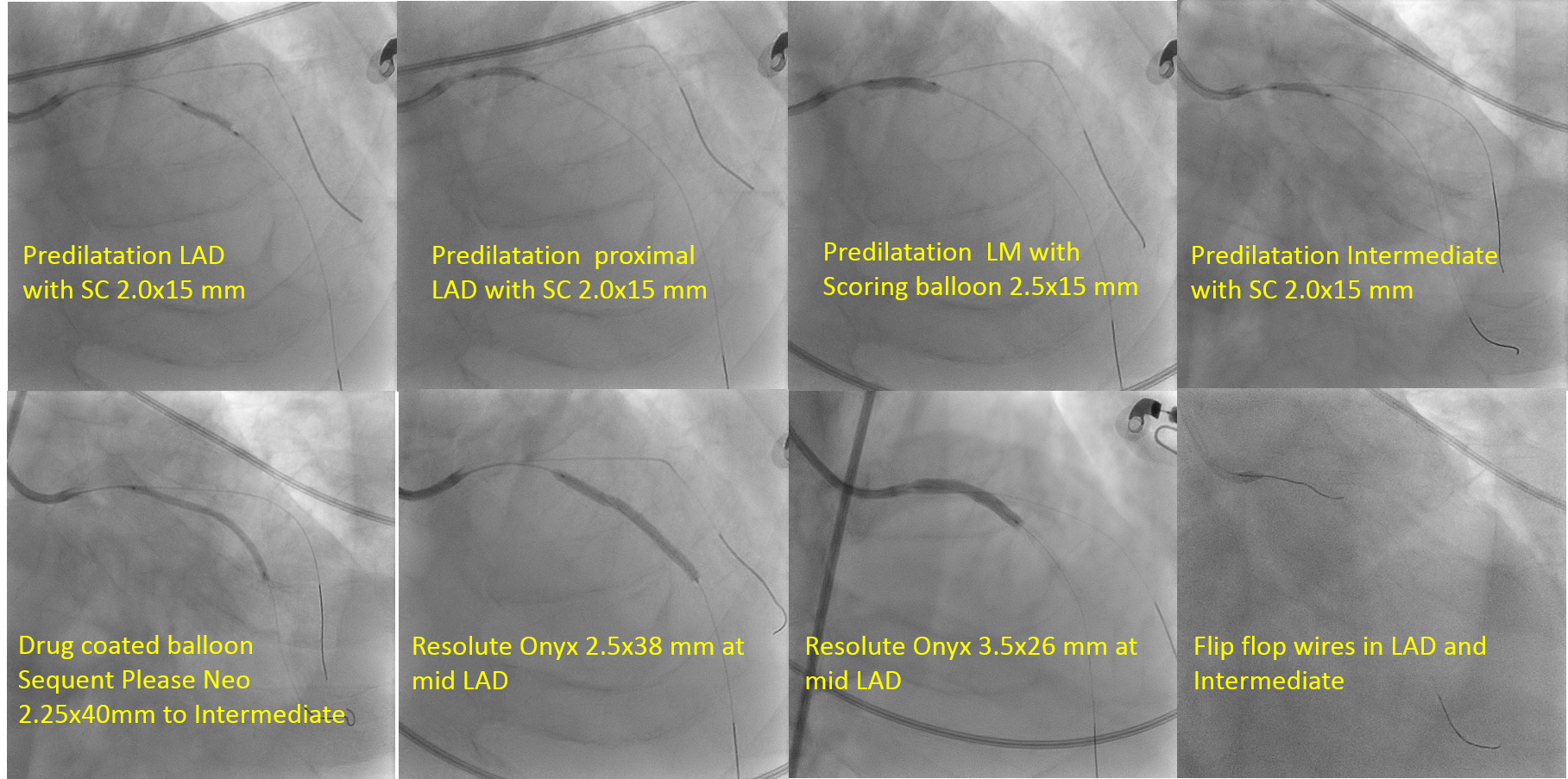
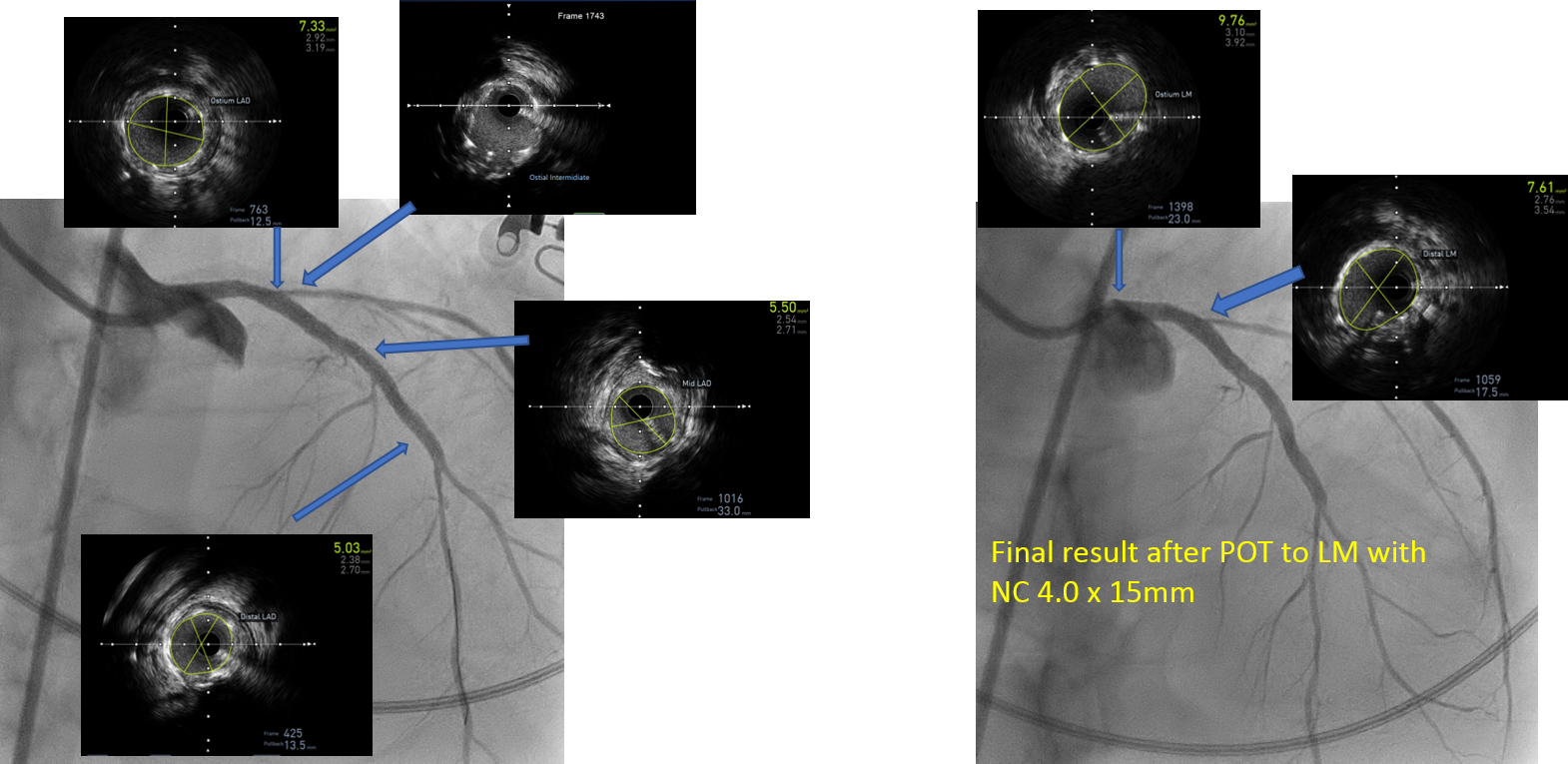
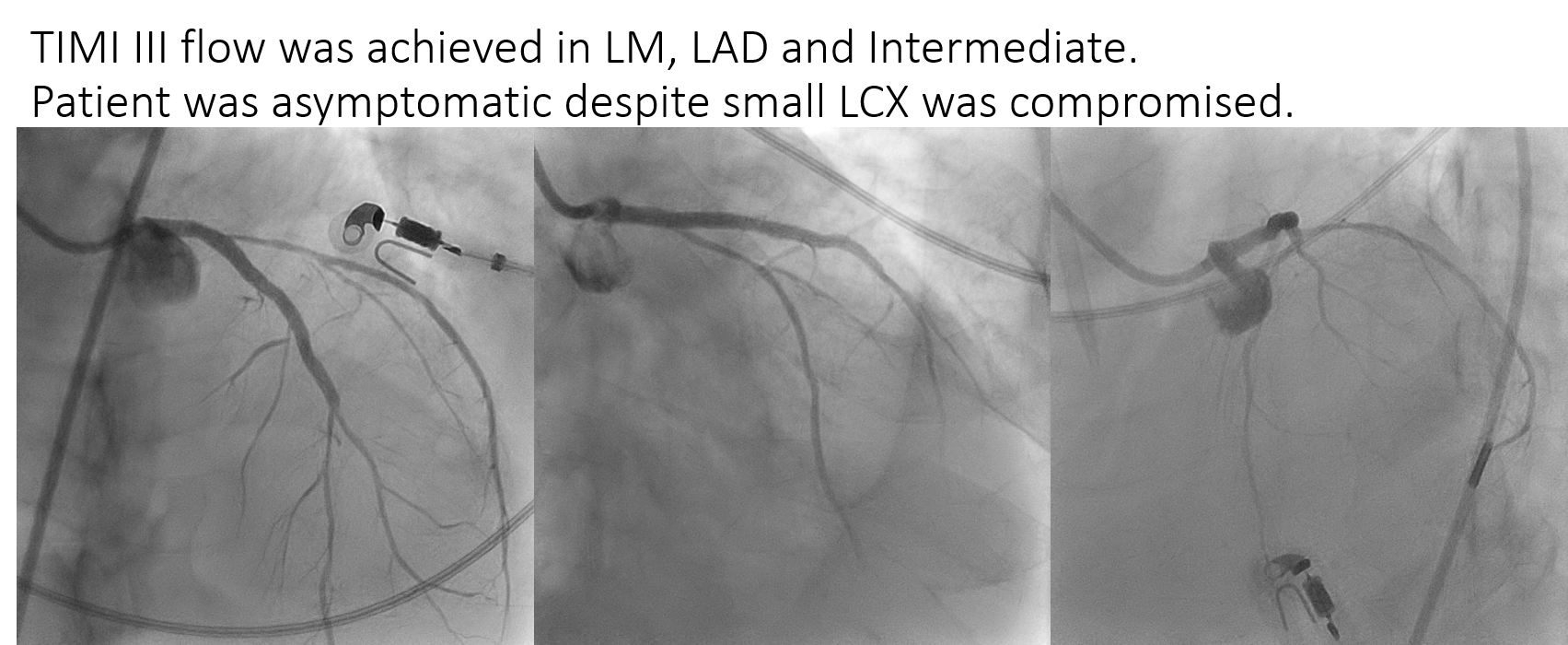
A 7 French sheath via right femoral artery and 8 French Sheath via left femoral artery were inserted. A 34 cc Intra-aortic balloon pump was inserted via left femoral artery. Judkins Left 4.0/7F catheter was engaged to LM then wired with a SION BLUE wire into the LAD and Runthrough Floppy wire to Intermediate. LAD was predilated with semicompliant SAPPHIRE II 2.0x15mm balloon at 6-8 ATM followed by SCOREFLEX NC 2.5x15mm at 14 to 18 ATM up to ostial LM in order to get better lesion preparation. The SAPPHIRE II 2.0x15mm was used to predilate the Intermediate. DCB Sequent Please Neo 2.25x40mm was delivered to Intermediate. ZES Resolute ONYX 2.5x38 mm and Resolute ONYX 3.5x26mm were delivered at mid LAD and LM to proximal LAD respectively. Postdilatation of LAD was performed with a non-compliant NC TREK balloon 3.0x15mm at distal & mid then SAPPHIRE NC 3.5x15mm at pLAD & LM at 20 to 22 ATM. Intravascular ultrasound revealed well apposed stent with an achievement of minimal luminal area 5.03 mm2 at Distal LAD, 5.5 mm2 at mid LAD and 7.3 mm2 at ostial LAD respectively. Hence, proximal stent optimization (POT) of LM was done with SAPPHIRE II NC 4.0 x15mm at 16-18AM, which positioned meticulously just proximal to ostial Intermediate. Repeated IVUS showed well apposed LM stent with MLA 9.7 mm2. There was no stent edge dissection and thrombus in the stent. TIMI III flow was achieved in LM, LAD and Intermediate. Patient was asymptomatic despite small LCX was compromised.
   - Case Summary:
Unprotected left main trifurcation lesion is the one of the most technically challenging procedures in interventional cardiology. In view of high bleeding risk in our patient, provision stenting with the single HBR approved stent and DCB was successfully performed in LM bifurcation lesion. Patient was stable during regular follow up.
|
|