Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200922_002
| Complications - Complications | |
| Catheter-induced Aortic Dissection During Coronary Stenting - Surgery or Intervention? | |
| David Baghdasaryan1 | |
| Nork-Marash Medical Center, Armenia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
B M
-Relevant clinical history and physical exam:
The 56-year-old man was admitted to the clinic for the planned stenting of the distal part of the right coronary artery (RCA). Anamnesis: Chronic obstructive pulmonary disease, arterial hypertension, active smoker, more than 20 cigarettes a day. By ECG T vawe inversion in leads II, III and aVF. By transthoracic echo EF=38%, hypokinesis of inferior wall. Blood test was normal, without any problems.
-Relevant test results prior to catheterization:
A month ago the proximal part of the RCA was re-stented by a BMS, in connection with the previously implanted stent thrombosis. On the left coronary system also had a diffuse atherosclerotic lesions.
 - Relevant catheterization findings:
Through the right radial access 6 Fr sheath was placed. Immediately after intubation with the AL 1 guide catheter of the RCA and injection of contrast medium, dissection of the ascending aorta (AA) was visualized. The patient had an hemodynamic instability, followed by a drop in blood pressure and severe chest pains began. Oxygen, fluids, and analgesia were administered.
|
|
|
[Interventional Management]
- Procedural step:
0.014″ soft-tip floppy Marker wire (BMW; Abbott Vascular,Santa Clara, CA, USA) unable to pass the RCA and after repeated contrasting, the RCA was completely occluded. AL 1 guide catheter was replaced by JR 4 and after this the guide wire was successfully advanced into the distal and after, the stenting of the aorto-ostial part was performed by 4.0 x 18 mm bare metal stent. The final result was satisfactory. In the RCA TIMI 3 flow and by angiography further signs of continuing dissection were not detected.
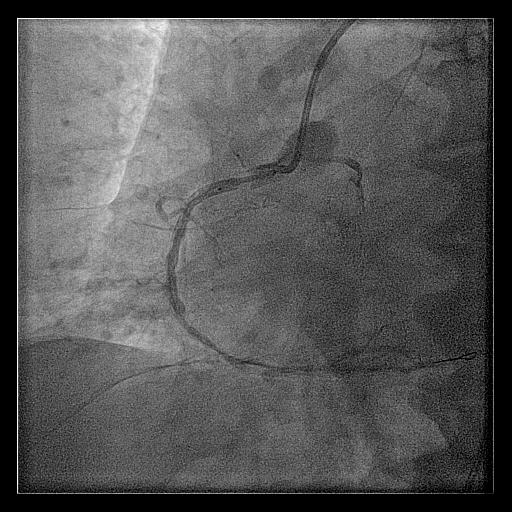 - Case Summary:
Iatrogenic aortic dissection of the ascending aorta (Type A) may be life-threatening, requiring surgical replacement of the diseased vessel, to avoid pericardial effusion, coronary artery dissection, or acute aortic regurgitation 1,2. According to our experience, retrograde dissection into the aorta during percutaneous coronary intervention (PCI) can be sealed with a coronary stent that covers the coronary ostium and should be treated conservatively in most circumstances, unless complication like extension of dissection into other vessels or pericardial effusion or hemodynamic instability occurs.
|
|