Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200921_004
| Complex PCI - Calcified Lesion | |
| Usefulness of Orbital Atherectomy to Superficial In-stent Calcified Plaques in Patients on Chronic Hemodialysis | |
| Kahoko Mori1, Hidehiko Nakamura1, Tetsuya Ishikawa2, Hideyuki Aoki1, Taro Takeyama2, Masatoshi Shimura2, Yuki Kondo2, Kota Yamada1, Yukiko Mizutani1, Itaru Hisauchi1, Shiro Nakahara1, Sayuki Kobayashi1, Isao Taguchi1 | |
| Dokkyo Medical University, Japan1, Dokkyo Medical University Saitama Medical Center, Japan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
K. N.
-Relevant clinical history and physical exam:
The indication of orbital atherectomy (OA) for heavily coronarycalcified plaques remained to be clarified by discriminating from rotationalatherectomy (RA). Superficial calcified plaques inside stent (in-stentcalcification: ISC) needed to be pulverized and broken prior to place stentinside in-stent restenosis (ISR).
-Relevant test results prior to catheterization:
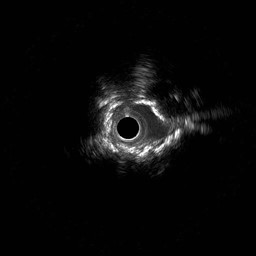
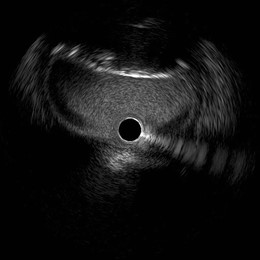
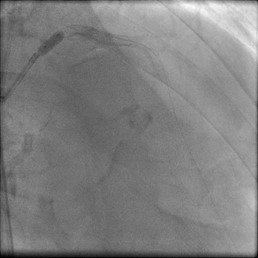
A 61-year-old male on chronic hemodialysis (HD) underwent PCI to ISCinside Xience stent placed in 2011 in mid-portion of left anterior artery (LAD)(Figures 1 and 2) and to convex calcified plaque in the oval ostium of leftmain coronary artery (LMCAos) (Figure 1 and 3). IVUS image revealed thesuperficial circular and irregular high-intensity plaque (ISC) in-side Xiencestent in mid LAD (Figure 2), and the eccentric convex-shaped superficialhigh-intensity calcified nodule at just LMCAos (Figure 3).
   - Relevant catheterization findings:
At first, in order to facilitate the procedure, LMCAos was dilatedby placing 3.5x18mm Synergy stent (Figure 4) with high pressure dilatation witha 4.5mm-sized non-compliant balloon at 20 atmospheres (Figure 5). OA wasselected for pulverizing ISC, because minimal lumen diameter of ISC was morethan 2mm (Figure 2). GuideWire was exchanged to ViperWire Advance.
   |
|
|
[Interventional Management]
- Procedural step:
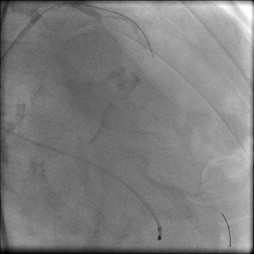
OA passed byante-grade and retro-grade approaches with low rotational speed for a few timeswithout evoking chest pain and ST-elevation. Then, atherectomy underwent byelevating rotational speed. Calcium surrounding from 8 to 1 o’clock was clearlypolished by OA, and OA broke the superficial calcified layer at 2 o’clock (Figure7), which made a following 3.5mm-sized balloon dilatations without indentationat 16 atmospheres (Figure 8). Synergy stent (3.5x20mm) was placed (Figures 9)without post-ballooning owing to well-apposed and almost symmetric dilation(Figure 10). Synergy stent at LMCAos fully obtained up to 12 mm2 (Figure 11).Therefore, PCI was ceased with good coronary flow from LMCA to LAD (Figure 12).
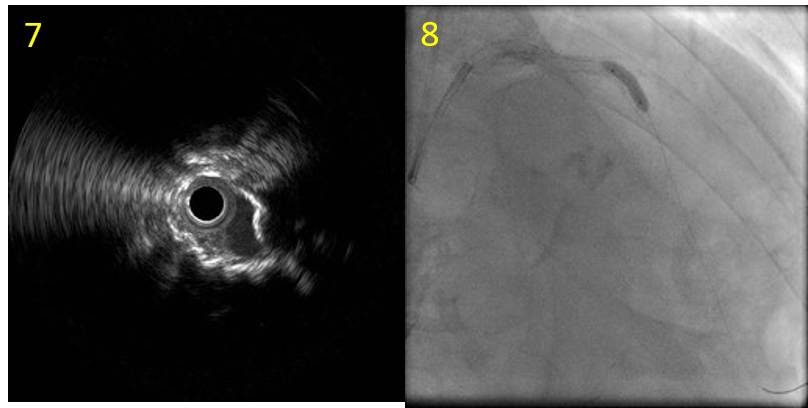 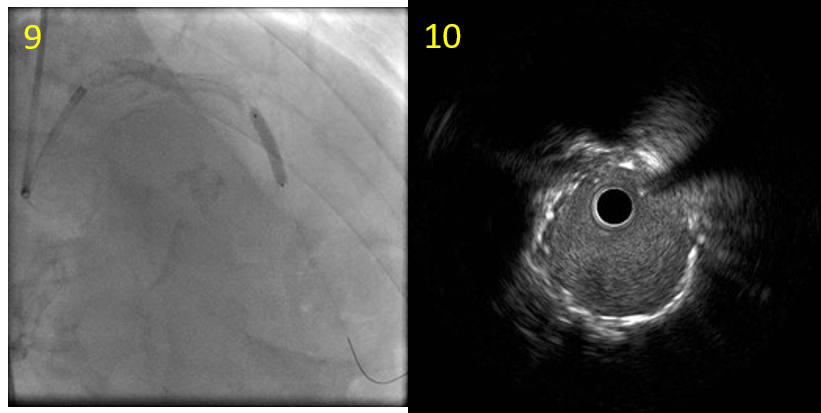 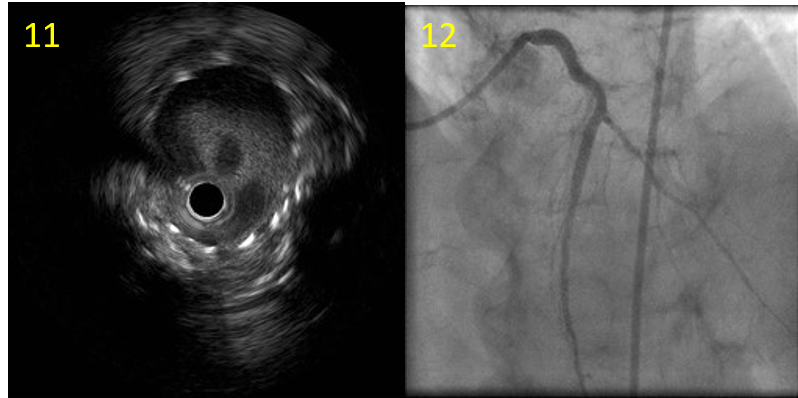 - Case Summary:
OA broke in thesuperficial layer (Figure 7). A 3.5mm-sized balloon was dilated withoutindentation (Figure 8), and 3.5mm-sized stent was placed (Figures 9).Post-ballooning was not conducted owing to the well apposition of Xience stent(Figure 10). Stent area at LMCAos was also obtained more than 8 mm2 (Figure11), with good angiogram of LMCA and LAD (Figure 12).
Conclusion: We present a case of9-year old ISC inside 2nd-generation drug-eluting stent successfullytreated with OA by modifying calcified plaque prior to place additional stentin a patient on HD. Thus, we confirmed that OA exerted the advantage over RAagainst calcified plaques with larger lumen including ISC. |
|