Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200921_003
| Imaging - Invasive Imaging (IVUS, OCT, spectroscopy, etc) | |
| Repetitive "Mimic In-stent Calcification" at Mid-Right Coronary Artery in Diabetes Patients on Chronic Hemodialysis | |
| Hideyuki Aoki1, Kota Yamada1, Tetsuya Ishikawa2, Taro Takeyama2, Kahoko Mori1, Masatoshi Shimura2, Yuki Kondo2, Yukiko Mizutani1, Hidehiko Nakamura1, Itaru Hisauchi1, Shiro Nakahara1, Sayuki Kobayashi1, Isao Taguchi1 | |
| Dokkyo Medical University, Japan1, Dokkyo Medical University Saitama Medical Center, Japan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
T.S.
-Relevant clinical history and physical exam:
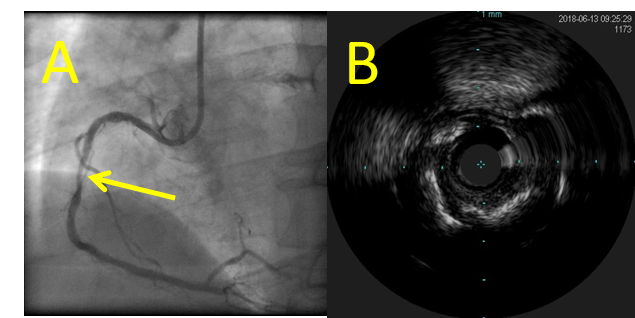
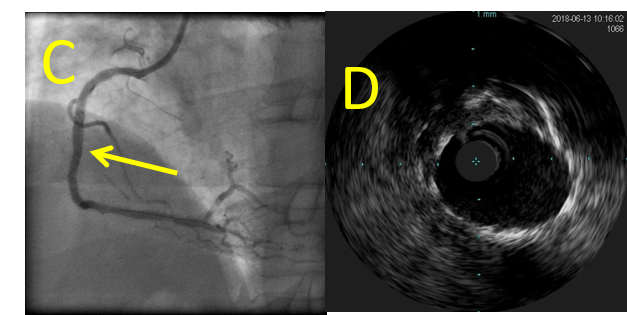
A 54-year-old male onchronic hemodialysis (HD), diagnosed as stable angina pectoris on old anteriormyocardial infarction, underwent percutaneous coronaryintervention (PCI) to diffuse moderatecalcified lesion in mid-right coronary artery (RCA) (A, B). At the initial PCI to RCA,Synergy biodegradable polymer everolims-eluting stent (3.5x38mm) was successfully placed withoutrotablator (C, D). His diabetic state was wellcontrolled, and dual antiplatelet therapy (DAPT) was continued.
  -Relevant test results prior to catheterization:
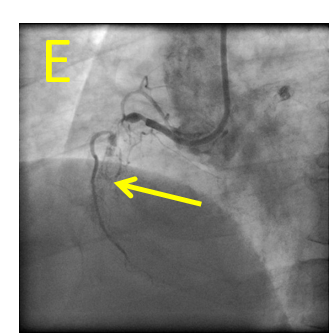
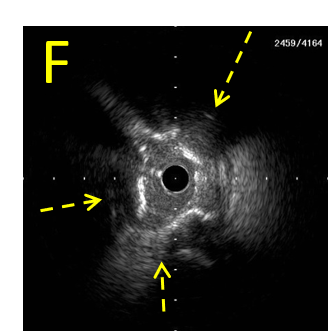
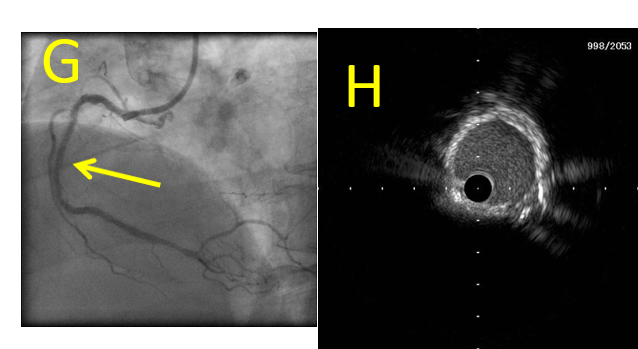
However, 8 monthlater, the secondary PCI underwent for in-stent occlusion (ISO) (E). IVUS imageat the primary stenotic site (indicated by yellow arrow in each figure) showed almostcircular superficial high-intensity layer with acoustic shadowing inside stent mimicking in-stentcalcification (ISC) (F, struts of expanded stent were indicated by yellowbroken-lined arrows). However, ISC in ISO was fully dilated by 3.5mm-sized non-compliantballoon and drug-coated balloon without indentation (G, H).
   - Relevant catheterization findings:
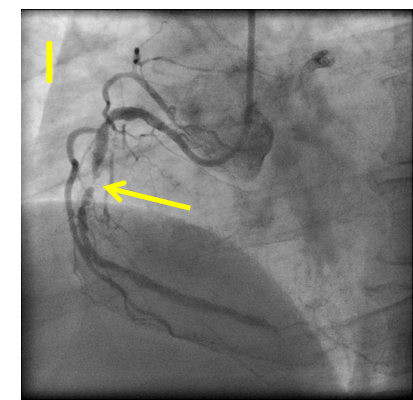
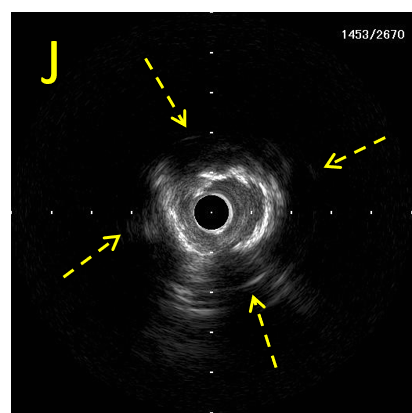
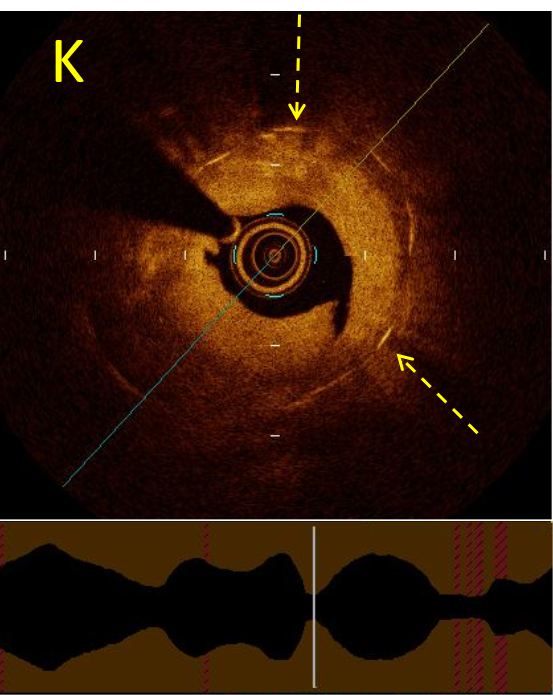
One-year later,however, severe in-stent restenosis (ISR) at the primary stenotic site was recurred(I) with recurrent superficial high-intensity layer (J). Opticalcoherence tomography (OCT) image showed layered neo-intimal pattern as high-backscattering growing mass with signalattenuation (seen in 4 to 9 o’clock) representing thick neo-intima growth inside Synergy stent, without characteristicsharp bordered low-intensity presentation of calcification (K).
   |
|
|
[Interventional Management]
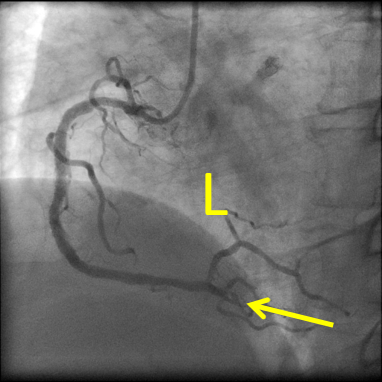
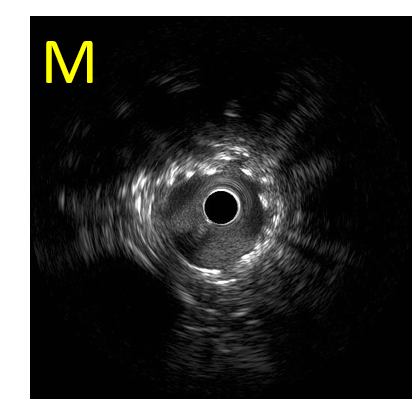
- Procedural step:
Because of the recurrence of superficialhigh-intensity layer, a biodegradable polymersirolimus-eluting stent (Orsiro 3.5 x 24 mm long) was placed inside Synergywith good expansion (L, M). ISC is usually necessary to modify by a rotablatorprior to ballooning and stenting because of severe advanced atherosclerosisdeveloped during a long-term1. The present repetitive superficial high-intensity layer complicated in early (< 12 months) ISR cases, and inpatients on HD, mainly comprised hyperplastic neo-intima easily to dilate.Therefore, we proposed the present superficial circular high intensity imagesby IVUS as “mimic ISC” by discriminating from ISC in view of balloonexpandability (H, M) and with layered in-stent restenotic OCT image withoutcalcification (K).
  - Case Summary:
ISC isusually necessary to modify by a rotablator prior to ballooning and stenting becauseof severe advanced atherosclerosis developed during a long-term1.The present repetitive superficialhigh-intensity layercomplicated in early (< 12 months) ISR cases, and in patients on HD, mainlycomprised hyperplastic neo-intima easily to dilate. Therefore, we proposed thepresent superficial circular high intensity images by IVUS as “mimic ISC” bydiscriminating from ISC in view of balloon expandability (H, M) and with layeredin-stent restenotic OCT image without calcification (K).
Conclusion: Since patients on HDwere the significant predictor of late (30-365 days) stent thrombosis in thepresent drug-eluting stent era, the features and the underlying mechanisms to develop“mimic ISC” during a relatively early phase should be clarified. |
|