Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200921_002
| High-Risk Intervention (diabetes, heart failure, renal failure, shock, etc) - High-Risk Intervention | |
| Usefulness of a Perfusion Balloon, Ryusei, for Intra-procedural Stent Thrombosis in Patients with Anterior ST-elevated Myocardial Infarction Complicated with Cardiogenic Shock | |
| Taro Takeyama1, Yukiko Mizutani2, Tetsuya Ishikawa1, Kahoko Mori2, Hideyuki Aoki2, Yuki Kondo1, Masatoshi Shimura1, Kota Yamada2, Hidehiko Nakamura2, Itaru Hisauchi2, Shiro Nakahara2, Sayuki Kobayashi2, Isao Taguchi2 | |
| Dokkyo Medical University Saitama Medical Center, Japan1, Dokkyo Medical University, Japan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
H. T.
-Relevant clinical history and physical exam:
Intra-procedural stentthrombosis (IPST) is a rare but seriouscomplication of thereperfusion therapy of acute myocardial infarction (AMI). However, detailpathophysiology and predictors of IPST, and the optimal method to treat IPSTwere not fully understood.
-Relevant test results prior to catheterization:
A 49-year-old male who presented withventricular fibrillation (VF) dueto anterior ST-segment elevatedacute myocardial infraction (STEMI) underwentemergency percutaneous coronary intervention (PCI) after return of spontaneouscirculation with intra-tracheal intubationand insertion of intra-balloon aortic pumping (IABP).
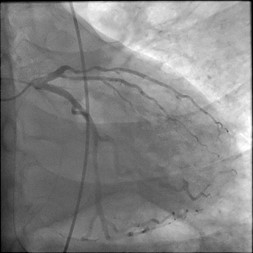
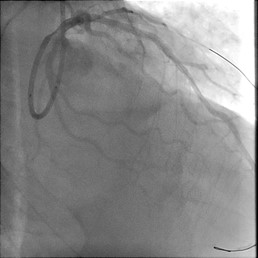
- Relevant catheterization findings:
The first angiogram revealedTIMI-0 grade flow at the proximal anterior descending artery (LAD) (Figure A). Following pre-dilations with 2 and 3 mm-sized semi-compliant balloons, an everolimus-elutingstent (Synergy 3.5 x 38 mm)was placed at the diffuse sclerotic culprit lesion from the mid to proximal LAD (Figure B). A few seconds after the stent implantation, diagonalbranch was occluded with thrombotic filling defect and thrombotic fillingdefect rapidly progressed to entire stent, i.e. IPST (Figure C).
   |
|
|
[Interventional Management]
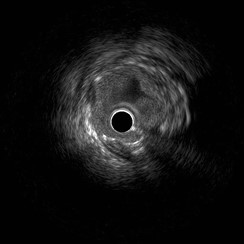
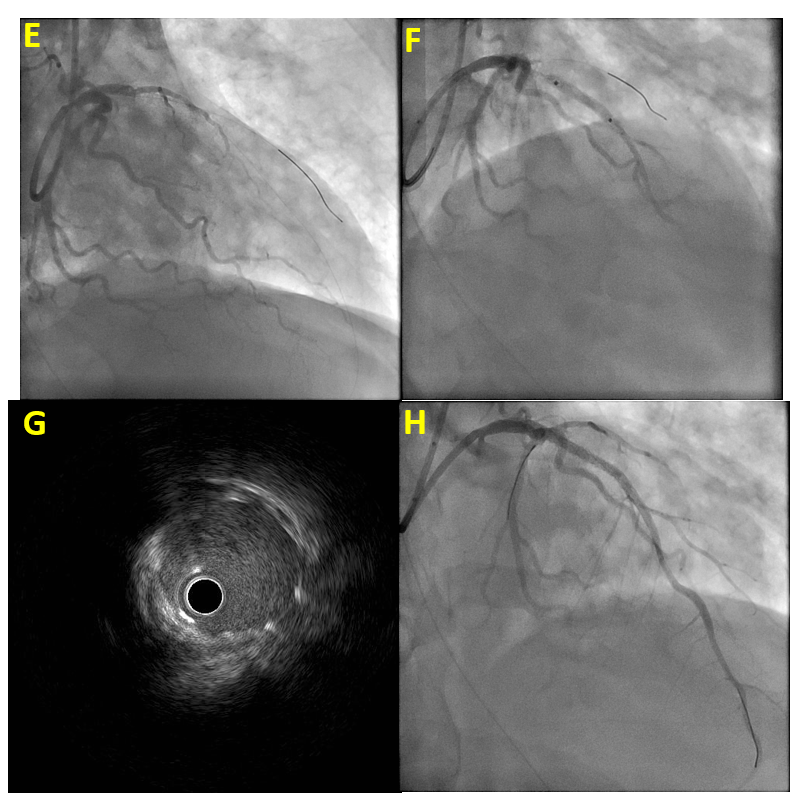
- Procedural step:
The activatedclotting time was over 200 s, and argatroban (10mg) was intra-coronaryadministered for a few times. With frequent aspirations for developed in-stentthrombus, a 3.5 mm-sized non-compliant balloon was inflated several times.However, it failed to manage thrombus, representing as a plenty of protrudedthrombus image by IVUS (Figure D), implicated in repetitive no-reflowphenomenon (Figure E). In addition, it was difficult to inflate long-timebecause of occurrence of VF. Then, weused a perfusion balloon (Ryusei 3.5 x 20 mm), enabled to inflate long-timewith maintaining coronary perfusion (Figure F). By repeated long-time andhigh-pressure perfusion balloon inflations, the final IVUS image showed thewell suppressed in-stent thrombus inside Synergy (Figure G). Then, PCI wasceased by obtaining TIMI-3 grade flow (Figure H).
  - Case Summary:
A perfusion balloon, Ryusei, enabled long-timeinflation without hemodynamic deterioration in the reperfusion of STEMI complicated withcardiogenic shock. Thus, long-time balloon inflationwith a perfusion balloon, Ryusei,deemed to be a valid option for intra-procedural stent thrombosis (IPST).
|
|