Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200910_004
| Complex PCI - Bifurcation/Left Main Diseases and Intervention | |
| Tip Detection Method Adapted for both CTO and Non-CTO Complex Lesions During IVUS-guided Coronary Intervention | |
| Kota Tanaka1, Atsunori Okamura2, Kenshi Fujii1 | |
| Sakurabashi Watanabe Hospital, Japan1, Sakurabashi Watanabe Advanced Healthcare Hospital, Japan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
M.S
-Relevant clinical history and physical exam:
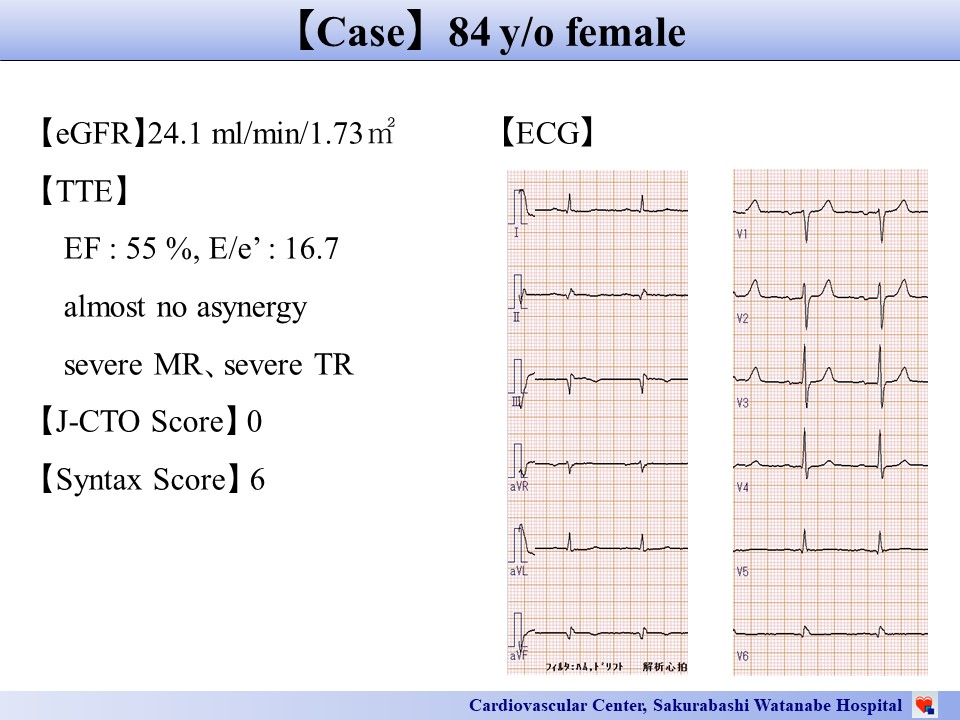
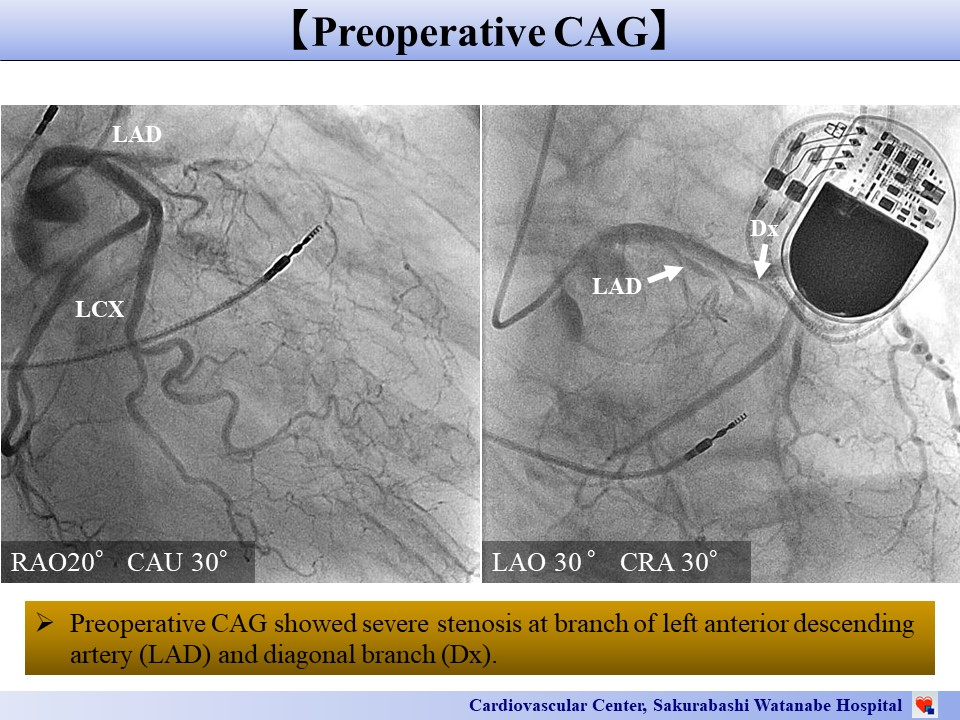
An 84-year-old woman visited our hospital to undergo heart surgery forsevere mitral and tricuspid regurgitation. Her baseline ECG was normal, and echocardiographyrevealed focal akinesis at inferior wall. Preoperative coronary angiography (CAG) showed occlusion in the proximal part of the left descending coronary artery (LAD) at the bifurcation site with a diagonal branch (Dx). Since there were good collaterals, the cardiac surgery was performed without the revascularizations to this lesion.
 -Relevant test results prior to catheterization:
The postoperative condition was good, but sepsis due to pneumoniaworsened general condition. At that time, new asynergy in the LAD region wasrecognized. Therefore, we performed percutaneous coronary intervention (PCI) toimprove her cardiac function via a right radial artery approach using a 7 Frsheath.
 - Relevant catheterization findings:
Preoperative coronary angiography (CAG) showed occlusion in the proximal part of the left descending coronary artery (LAD) at the bifurcation site with a diagonal branch (Dx).
 |
|
|
[Interventional Management]
- Procedural step:
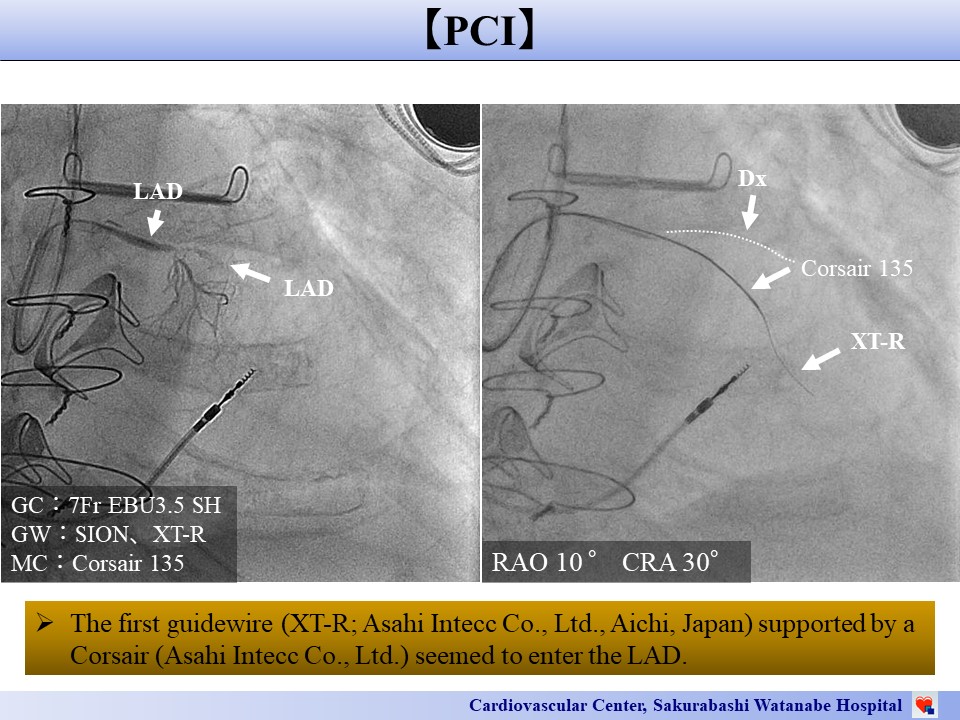
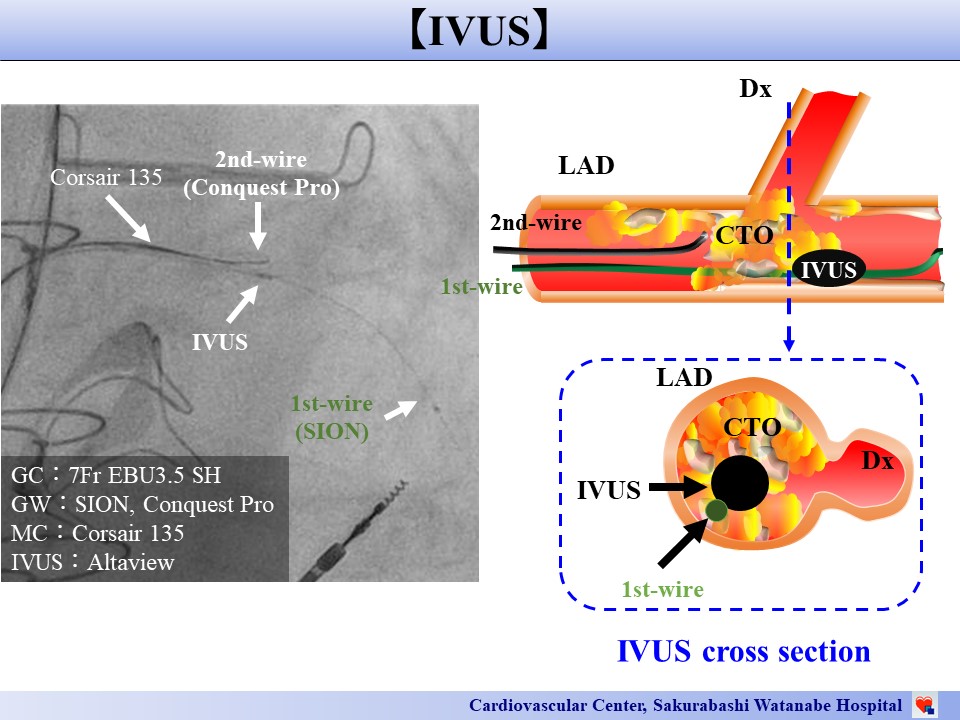
The first guidewire (XT-R; AsahiIntecc Co., Ltd., Aichi, Japan) supported by a Corsair (Asahi Intecc Co., Ltd.)entered the CTO lesion in the LAD. IVUS examination showed that there was a plaquebetween the root of the guidewire in the LAD and the entrance of the Dx. Therefore, weperformed the IVUS guided wiringusing the tip detection method to advance the second guidewire (Confianza-12g;Asahi Intecc Co., Ltd.) accurately toward the entrance of the Dx. IVUS examination fromDx revealed that there was a plaque between the guidewire in the Dxand the guidewire in the LAD. If we had dilated the lesion in this situation, the plaque shift wouldhave occluded either branch. The route of the guidewire in the Dx was connectedto the LAD main branch, but there was a steep curve on this route. Although we performed the parallel wire technique and the reverse wire technique using a dual lumen catheter, guidewires could not be passed through the route to the LAD mainbranch. Therefore, we moved ontothe tip detection method again and the secondguidewire could be advanced to the LAD main branch through this route. A stent wasimplanted only at the LAD main branch and normal antegrade blood flow was achieved both in the LAD and the Dx branches.
   - Case Summary:
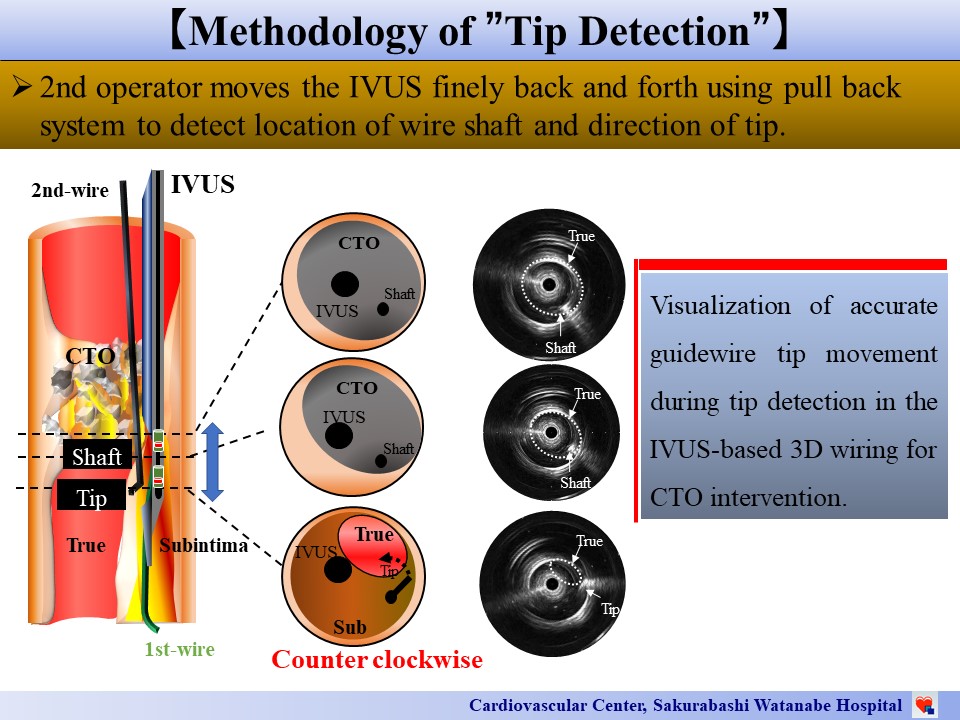
We first showed that the tip detection method was useful not only duringCTO PCI but also during non-CTO PCI because visualization of the 3D image enabledaccurate navigation of the guidewire even through routes where it was difficult for theguidewireto pass.
|
|