Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200910_003
| Complications - Complications | |
| Guidewire-induced Distal Coronary Perforation Management Using a Piece of the Coronary Balloon | |
| Seyedhossein Alavi1 | |
| Namazi, Iran1, | |
|
[Clinical Information]
- Patient initials or identifier number:
033556
-Relevant clinical history and physical exam:
A 49-year-old hypertensive female who had undergone primary PCI due to anterior ST-segment elevation myocardial infarction 4 weeks earlier, was referred to our hospital for PCI on posterior descending and right coronary arteries. Systolic and diastolic blood pressure was reported to be 150/90 mm Hg. Physical examination was unremarkable.
-Relevant test results prior to catheterization:
Baseline laboratory parameters were within normal limits. The assessment of 12-lead electrocardiogram showed normal sinus rhythm with deep T wave inversion in anterior and inferior leads due to prior myocardial infarction. Echocardiogram revealed wall motion abnormality in anterior and septal area with left ventricular ejection fraction of 50%.
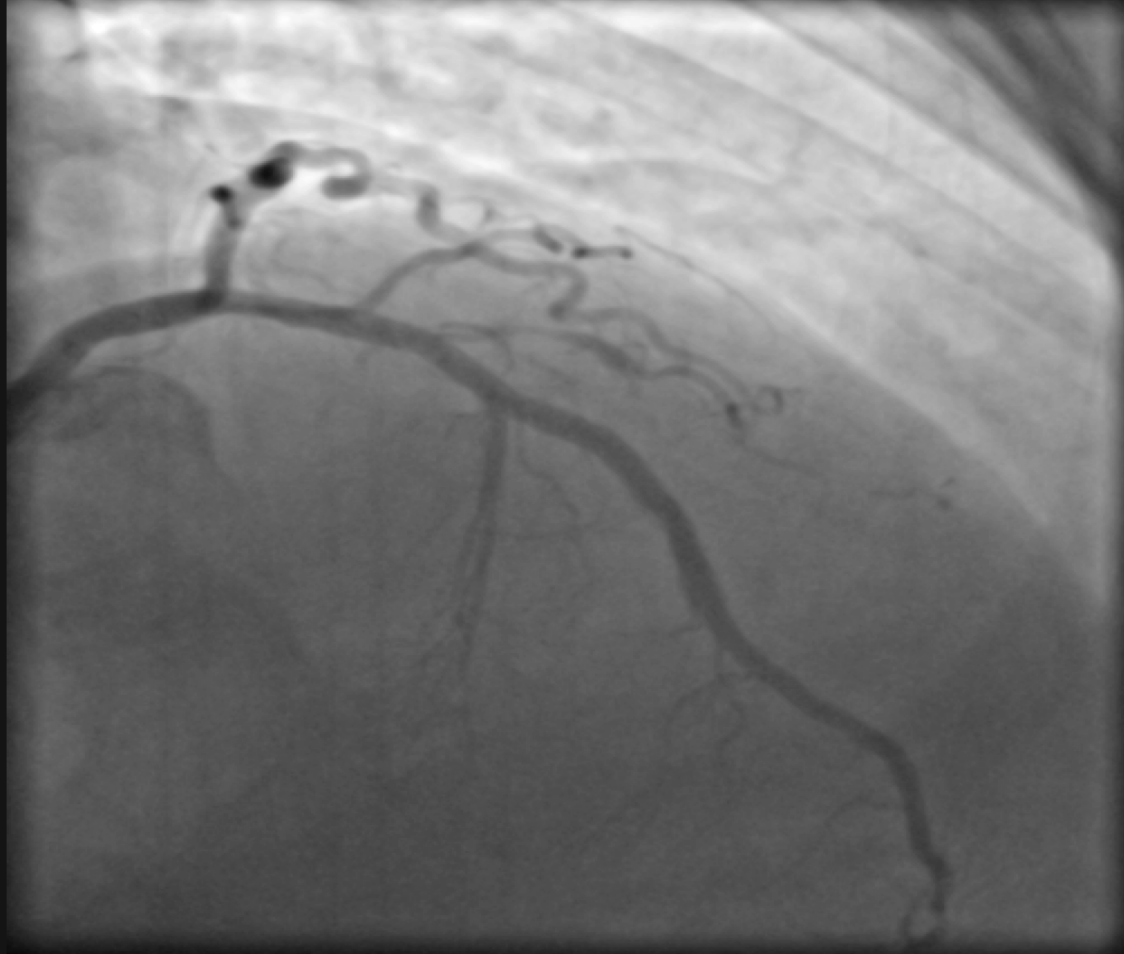
- Relevant catheterization findings:
In baseline coronary angiography, patent prior left anterior descending artery stent, normal circumflex artery and severe stenosis in the mid-part of right coronary artery and posterior descending artery were detected.
  |
|
|
[Interventional Management]
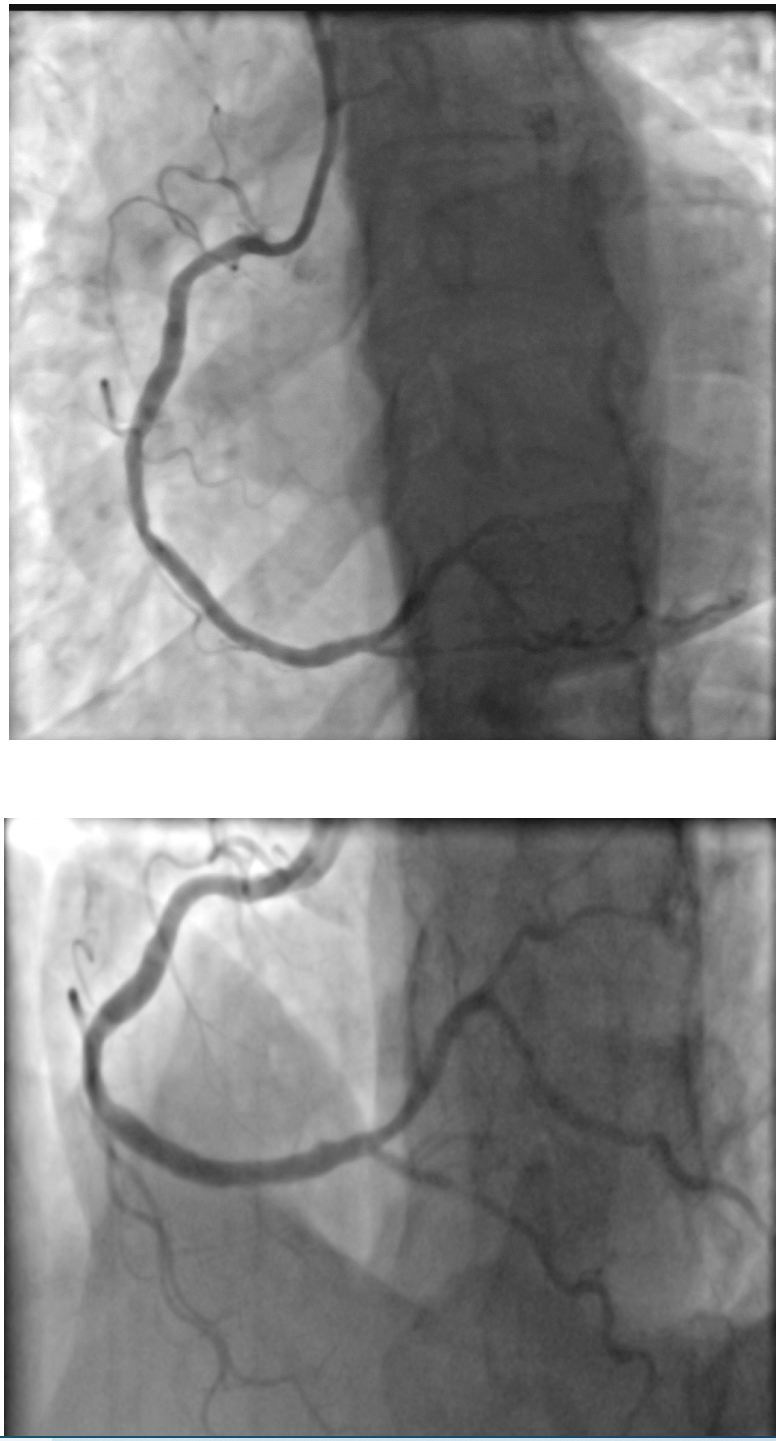
- Procedural step:
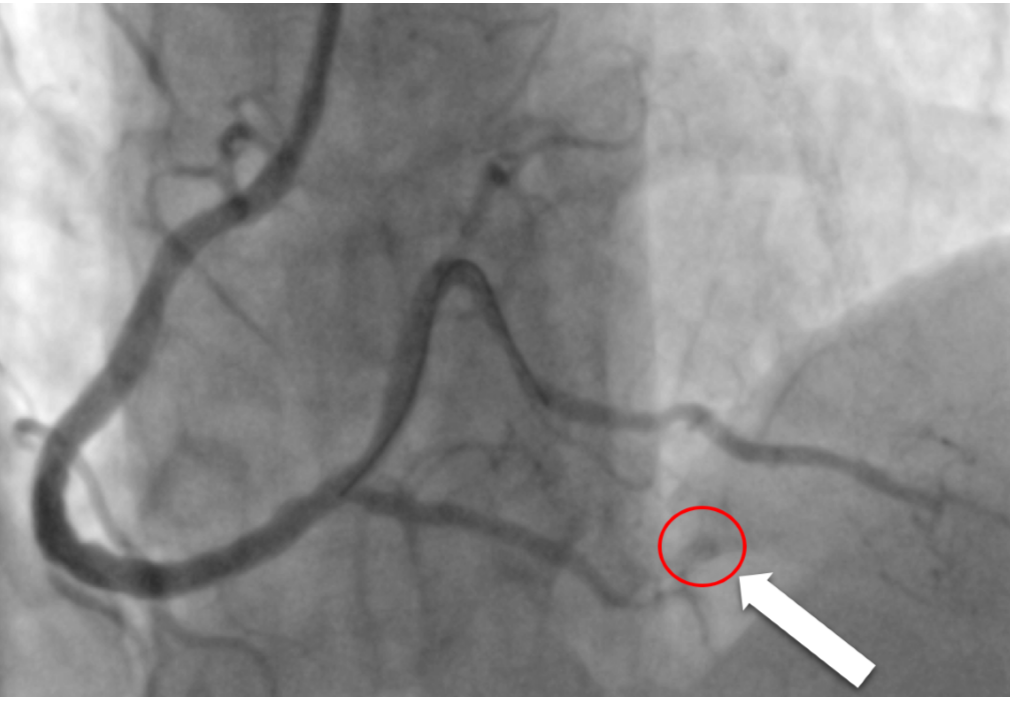
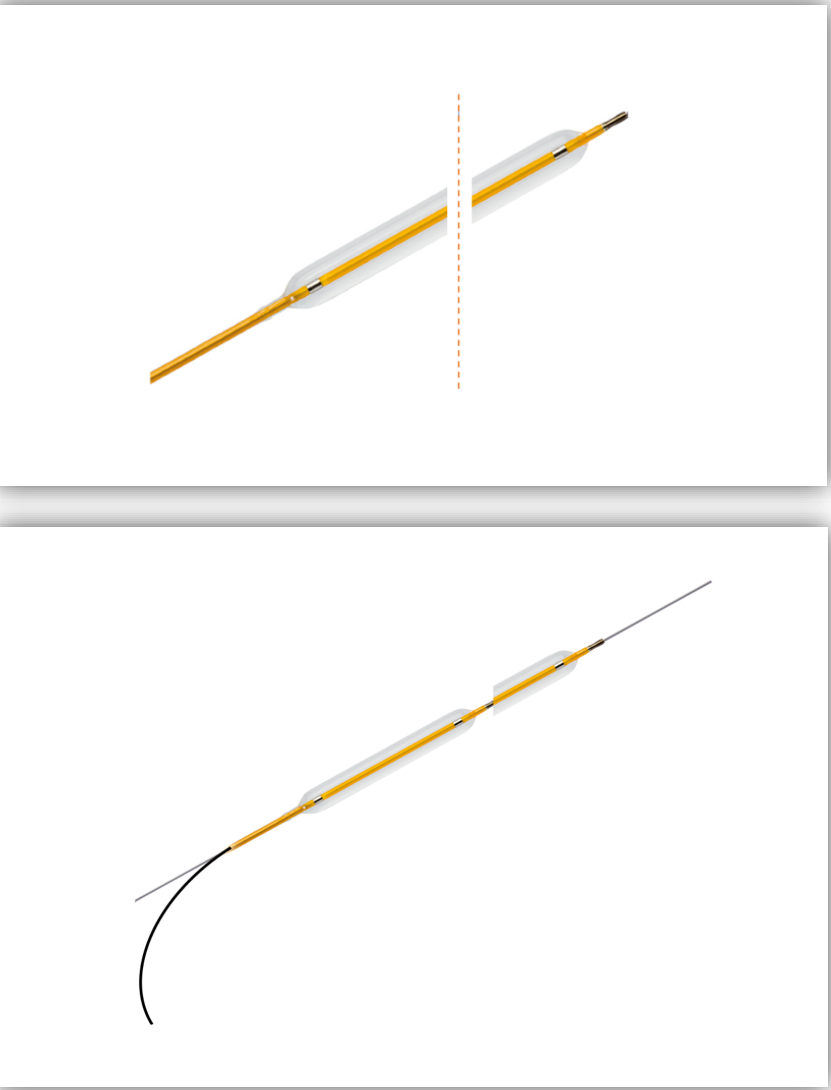
A 6-French Judkins right guiding catheter was advanced into the right coronary artery ostium. 8000 international units of heparin was administrated. The 0.014 guidewire was passed through right coronary and posterior descending arteries. Pre dilatation of posterior descending artery was done, but 2.25×16 Promus Premier drug eluting stent did not cross through PDA lesion. Buddy wire with 0.014 Balanced heavy weight guidewire was performed and the stent was crossed and deployed. There was a guidewire induced distal dissection without flow limitation. We deployed a 4×22 Orsiro drug eluting stent in the mid part of the right coronary artery. A small wire perforation as well as a dissection was detected in PDA. Low pressure balloon tamponade was done several times to no avail. Autologous fat taken from femoral area was embolized, but it was not effective. We then embolized clotted autologous blood with no success. There was no coil or Gelfoam available. We cut a part of the 3×15 Apollo catheter and kept two third of the balloon’s distal part. After placing this piece of balloon on the wire, e pushed that balloon particle along the guidewire with a new 2.75×15 Apollo balloon catheter towards the perforation. The guidewire was withdrawn into the balloon and the distal balloon particle was embolized into the PDA. The blood leakage caused by the perforation was decreased. Therefore, we once more followed through the above. Finally the perforation was sealed with two pieces of balloon.
 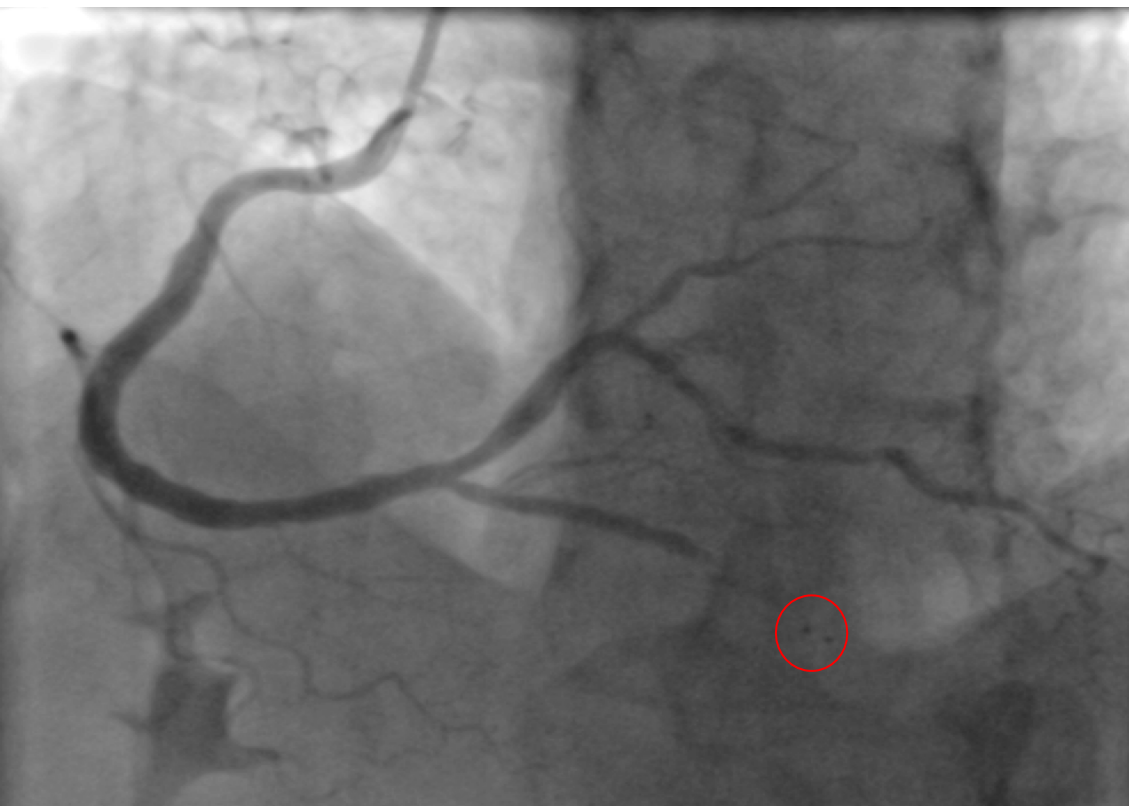  - Case Summary:
Overall, Distal coronary perforation caused by guidewire is a very rare, however extremely lethal complication and needs immediate intervention. In this case report we represented a new method; balloon embolization. This is an effective method which can be used in all cath labs and requires close to no special equipment. There is no need for anything special and It can be done in all cath labs with different levels of technology. The benefits of this method: it is cost efficient and no special equipment or qualities is needed. Also there is no need to remove the guidewire and several pieces of balloon can be embolized until the bleeding has stopped
|
|