Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200824_001
| Complex PCI - Chronic Total Occlusion | |
| The Hidden Highway | |
| Thinnakrit Sasiprapha1, Krissada Meemook1, Mann Chandavimol1 | |
| Ramathibodi Hospital, Thailand1, | |
|
[Clinical Information]
- Patient initials or identifier number:
PK
-Relevant clinical history and physical exam:
The 53 years old man with type 2 DM presents with chest pain for three months. The pain was located at the left chest wall, radiated to the left arm, aggravated by exertion and relieved by rest. He had a positive exercise stress test from the referral hospital and was referred for coronary angiography. His cardiovascular examination was normal.
-Relevant test results prior to catheterization:
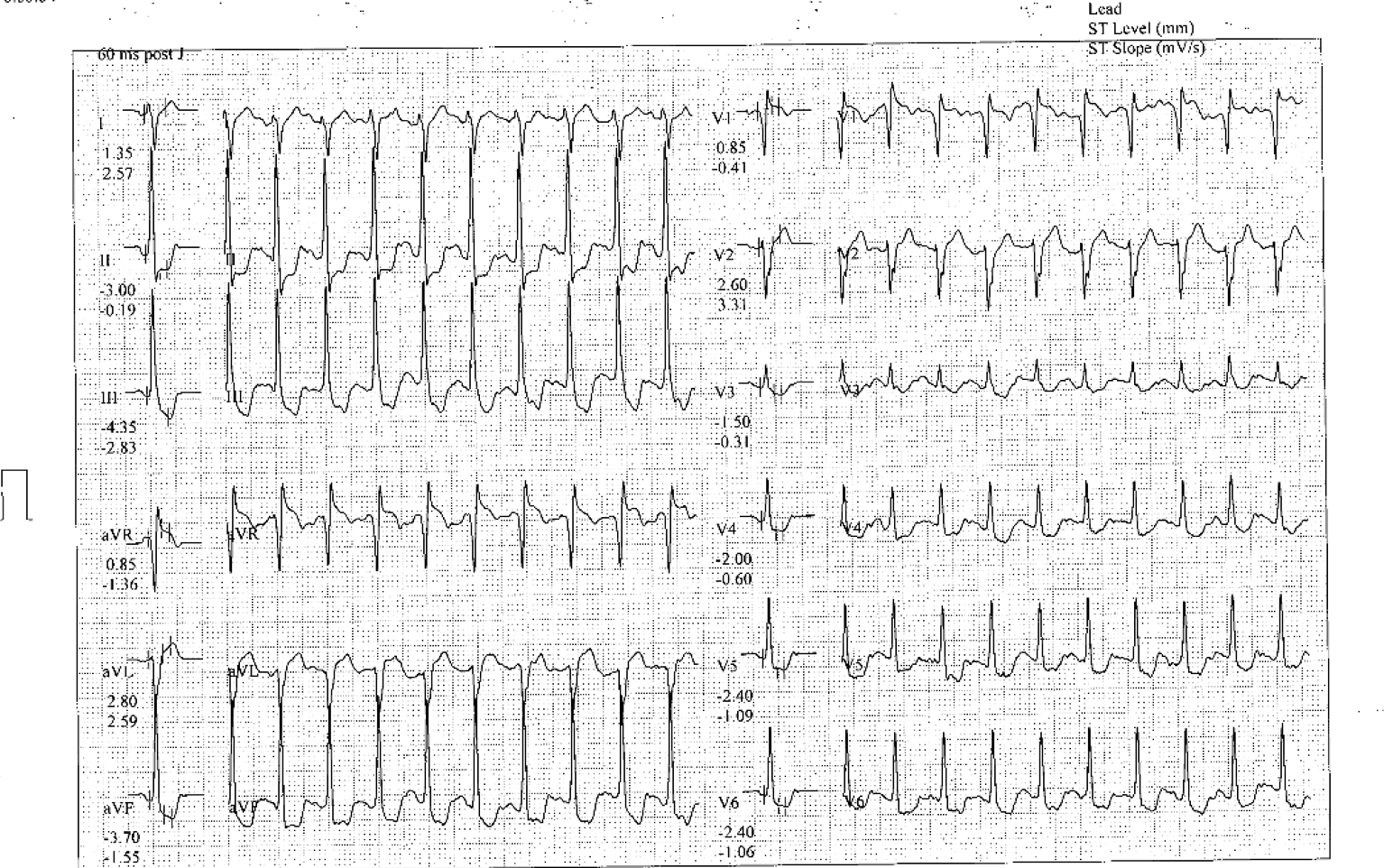
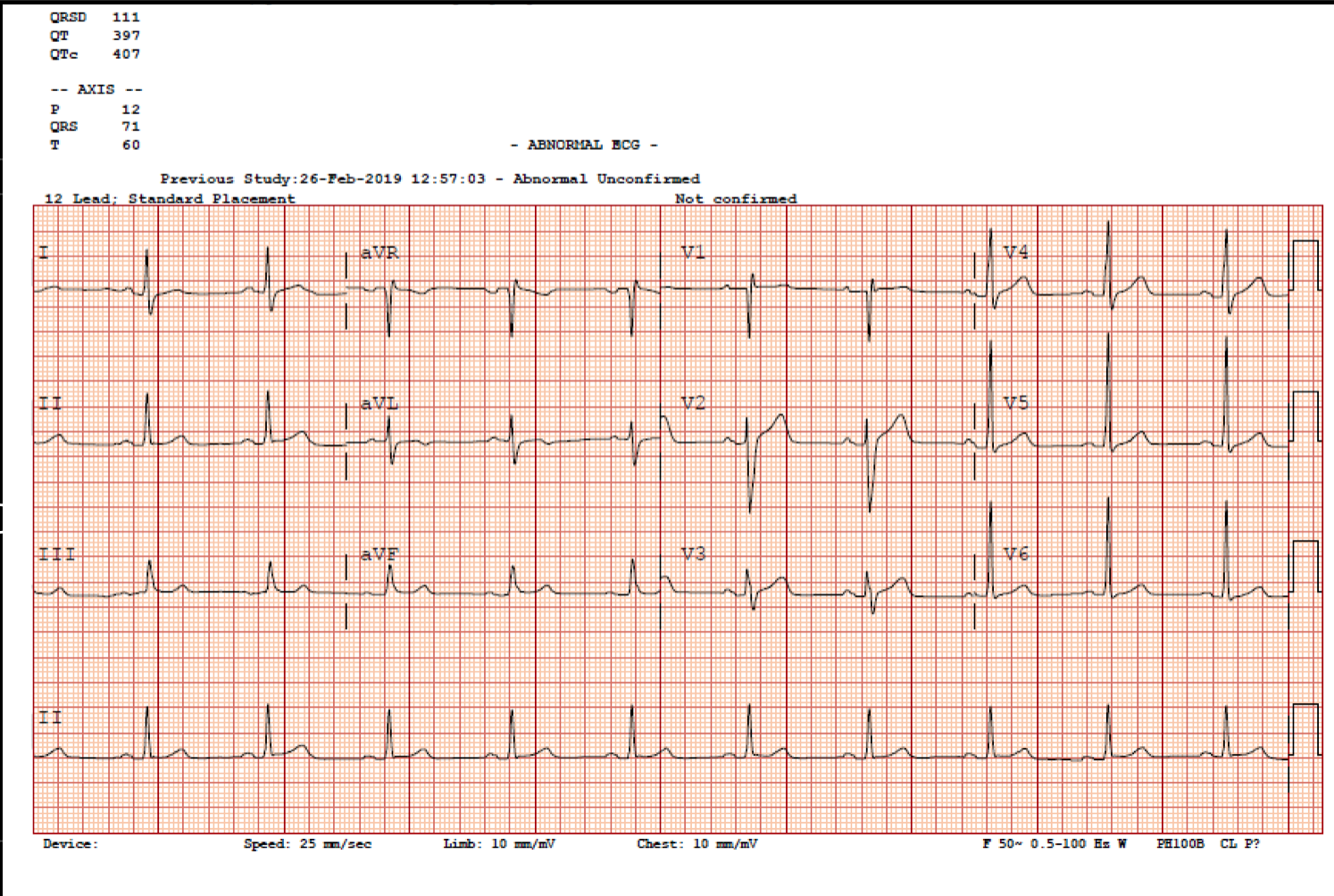
His resting EKG was within normal, but the stress ECG test showed deep down-sloping ST depression at III, aVF and V4-6 during the maximal exercise test. He achieved a work level of METS 8. He had a normal heart rate response and blood pressure response during the test. The resting echocardiogram showed normal LV systolic function (LVEF 67%) without wall motion abnormalities.
   - Relevant catheterization findings:
Coronary angiography via right radial artery access revealed a right dominant system, there was chronic total occlusion at mid LAD just after giving a large diagonal branch. There was no significant stenosis in other vessels and LAD was given collaterals from RCA, predominantly from the conus branch.
|
|
|
[Interventional Management]
- Procedural step:
The RCA was engaged with guiding JR3.5 via right radial artery access. A Corsair microcatheter was passed to the conus artery and a selective injection was done to reveal the collaterals (Vieussen's ring). A simultaneous coronary injection showed a short CTO segment at mid LAD. We successfully wire through the CTO by Fielder FC wire supported by a Finecross microcatheter. A semi-compliance balloon 1.5 mm was inflated at the lesion and a subsequent angiogram revealed the severe stenosis at mid LAD-DG bifurcation (Medina 1,1,1). A Sion blue wire was crossed to the DG-2. An IVUS showed the proximal main branch, distal main branch and side brach sizes were 3.5 mm, 3.0 mm and 2.75 mm respectively. We decided to do a Culottes technique. We deployed the first stent (EES 2.75 x 32 mm) at LAD-DG-1 and then did the first POT with 3.5 NC Balloon at the proximal main branch and the wire exchanged was done. The IVUS confirmed that a wire crossed to the distal strut to the distal main branch. We opened the strut to the distal main branch with a 2.5 mm semi-compliance balloon. The second stent (EES 3.0 x 20 mm) was deployed at the main branch. The side branch wire was recrossed. A post-dilatation was done with a 3.0 mm NC balloon and 2.75 mm NC balloon at the distal main branch and side branch respectively followed by kissing balloon inflation. The second POT was done with a 3.5 NC balloon at the proximal main branch. The final angiogram and IVUS showed good results.
- Case Summary:
We successfully treated the case with chronic total occlusion and bifurcation lesions. The learning points from this case were, first, selective injection with a microcatheter via conus branch can give excellent and clear collateral to LAD and also decreases the amount of contrast usage. Second, an IVUS is helpful for planning and stent optimization in the bifurcation lesion.
|
|