Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200810_001
| Complications - Complications | |
| When Every Step is Complicated, a Case of Double Kissing Crush Primary Percutaneous Intervention | |
| Mohammed Ali Osheiba1, Sohail Khan2 | |
| Queen Elizabeth Hospital Birmingham, United Kingdom1, Queen Elizabeth, United Kingdom2, | |
|
[Clinical Information]
- Patient initials or identifier number:
S L
-Relevant clinical history and physical exam:
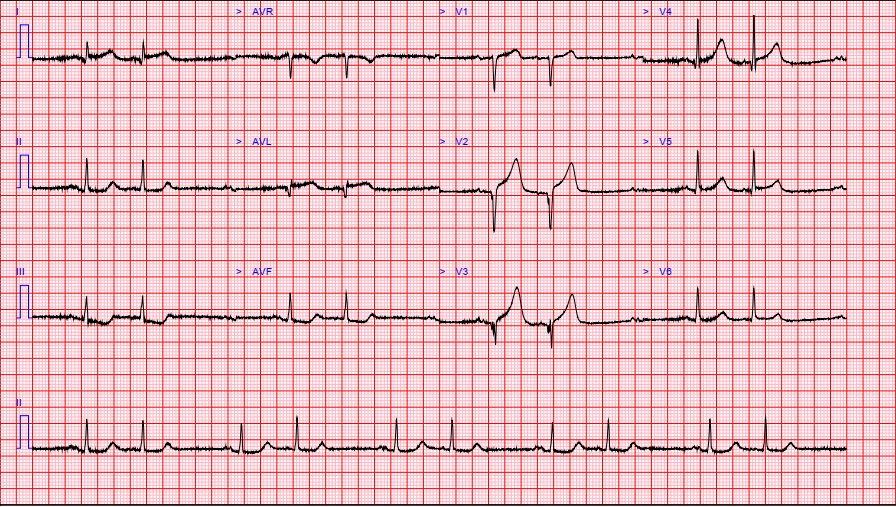
A 66-year-old gentleman with a past history ofhypercholesterolemia and multiple sclerosis presented with chest pain whilst hewas walking followed by collapse with brief loss of consciousness. His ECGshowed ST elevation in anterolateral leads.
 -Relevant test results prior to catheterization:
- Relevant catheterization findings:
LAD was full of thrombuswithTIMI 1 flow,1st diagonal (D1) was totally occluded  |
|
|
[Interventional Management]
- Procedural step:
• LAD was wired with Runthrough wire and dilated with 2.5 x15 balloon,TIMI flow improved • Wiring of D1 with Runthrough wire and pre-dilation with 2 x 12 Balloon• Extensive disease in diagonal with thrombus therefore we decided toproceed to DK crush stenting of LAD and D1• D1 stented with 2.5 x24• Crush performed with 3.0 NC• Rewiring of D1 with a whisper MS and 1st Kissing ballooninflation with 2.5 and 3.0 in the diagonal and LAD respectively. • No-reflow in D1, therefore Integrillin administered• Further Balloon dilation of diagonal stent to restore flow• Stenting of LAD with 2.5 x 24 and 3 x 38• LAD was optimised with 3.5 NC balloon but there was poor distal flow andlikely outflow dissection and 3rd overlapping 2.5 x32 was deployed • There was very good LAD flow and TIMI 3 flow was established• POT of LAD and Final Kiss performed• At this point we noted extravasation of contrast due to distalperforation of the diagonal• Patient was haemodynamically stable, immediate echo did not show apericardial effusion• Balloon tamponade was performed for 15min but unsuccessful
- Case Summary:
In this casewe experienced 3 complication, edge dissection, thrombotic occlusion ofdiagonal and wire perforationIt isimportant to ensure that the distal wires are well visualised during a complexPCI case especially if hydrophilic wires have been usedOthertreatment options for sealing a perforation include clotted blood, or fatembolization, here we used dedicated micro-coils
|
|