Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200409_001
| CORONARY - Complications | |
| Difficult Catheter Engagement Due To Protruding Aorto-Ostial Stent: How Self-Shaping Catheter Overcame the Challenge | |
| Kuo Ting Lee1, Dharmaraj Karthikesan2, Chea Chin Yung3, Saravanan Krishinan4, Chee Tat Liew5 | |
| Sultanah Bahiyah Hospital, Malaysia1, Hospital Sultanah Bahiyah, Malaysia2, HSB, Malaysia3, Ministry of Health Malaysia, Malaysia4, Pantai Penang Hospital, Malaysia5, | |
|
[Clinical Information]
- Patient initials or identifier number:
SAK 00800837
-Relevant clinical history and physical exam:
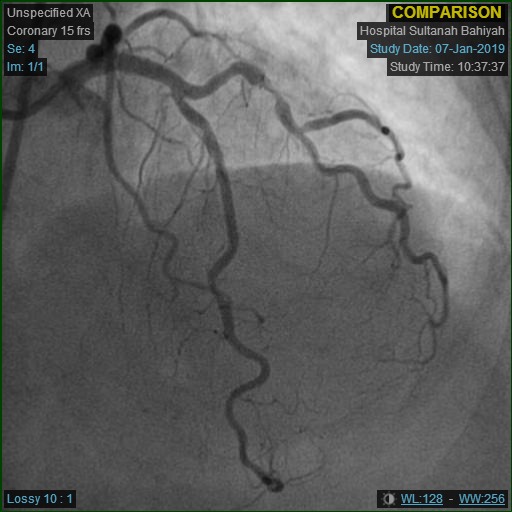
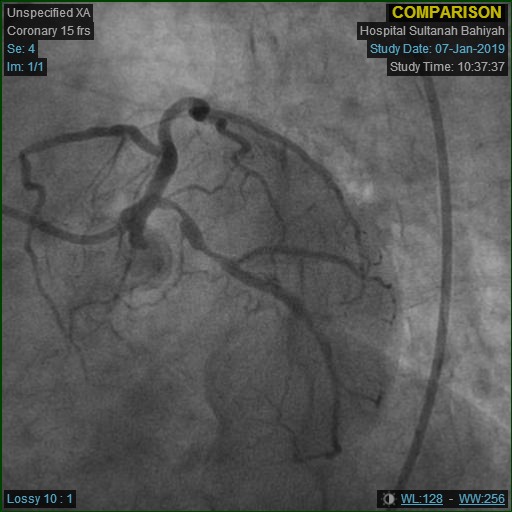
SAK, 71, lady, had history of hypertension and ischaemic heart disease. Coronary angiogram in Jan 2019 showed triple vessel disease. Ad hoc PCI to RCA was performed , of which the ostial 80-90% stenosis was stented with DES 3.0x28mm. LCX and LAD/D1 lesions were planned for staged PCI. Unfortunately the procedure was delayed while patient developed new onset angina, 14 months after the index procedure. LVEF: 52%.
  -Relevant test results prior to catheterization:
  - Relevant catheterization findings:
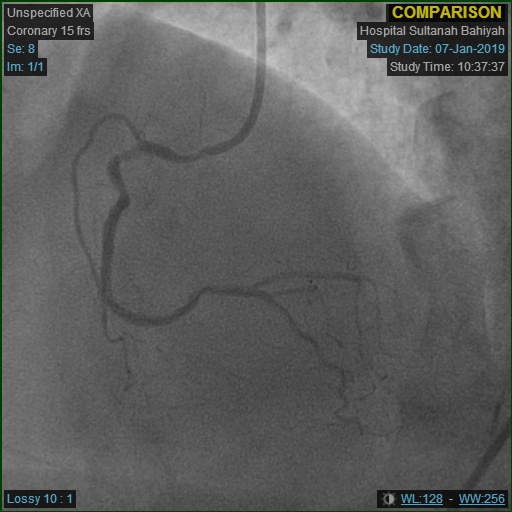
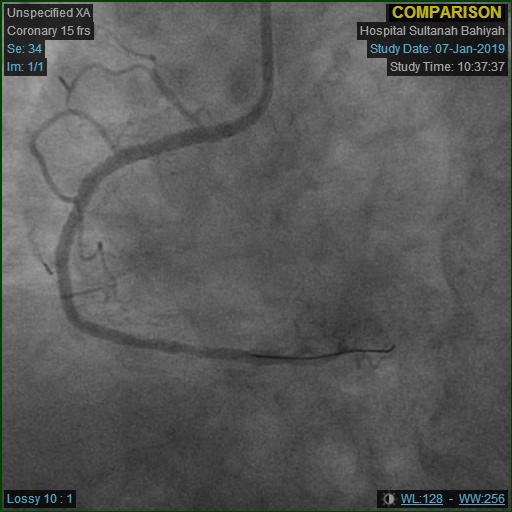
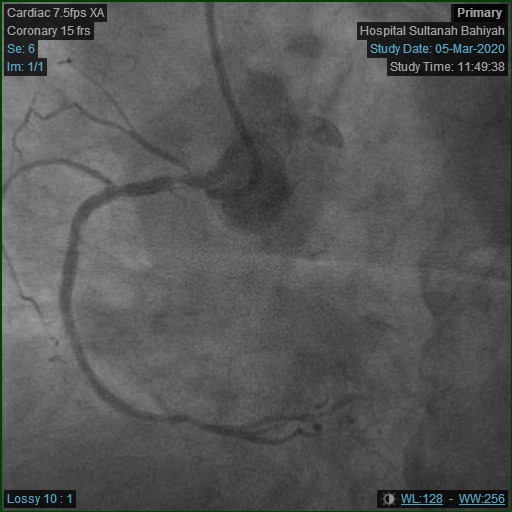
Repeat angiogram was done via right radial approach. Yet, a 6Fr JR3.5 diagnostic catheter failed to engage RCA due to overhanging struts from previous ostial stent. Alternatively, a near-ostium non-selective injection was taken. Previous stent revealed Focal Instent Restenosis of 70-80% (Type 1C) at proximal segment. Left-sided vessels were unchanged: LCX proximal 80-90%, LAD moderate disease and significant diagonal lesion.
   |
|
|
[Interventional Management]
- Procedural step:
Strategy was planned for IVUS interrogation to RCA ISR before intervention.
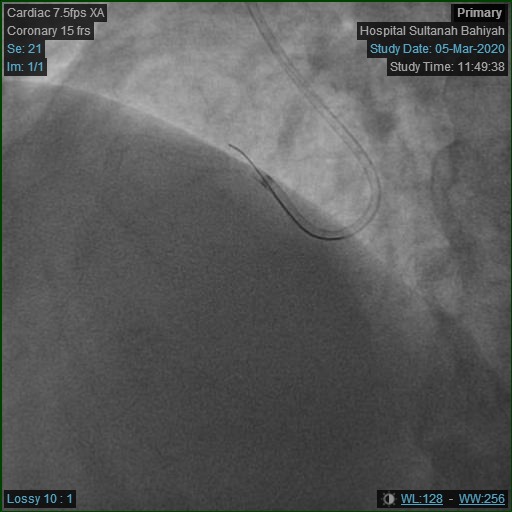
However, RCA engagement with 6Fr JR3.5 guiding catheter was unsuccessful, despite switching to femoral approach. Multiple catheters were tried but failed to make progress, eg: JR4.0, Amplatz Left-1 (AL-1), Short Amplatz Left-1 (SAL-1). Further attempts were made to manipulate hydrophilic wires through the vessel lumen or across stent struts, which again yielded no resolution. Procedure was interrupted to examine the neo-RCA ostium constructed by the protruding struts. The effective ostium had shifted anteriorly by comparison, and the overhanging stent hindered any catheter engagement from rotational manipulation by torquing. Hence, a 6Fr JR3.5 catheter was refashioned to mimic the third curvature provided by the 'non-torque' SRC Williams Right Catheter, which shifted the catheter tip anteriorly beyond the existing plane of the primary and secondary curves. This allowed direct co-axial cannulation to take place without much torquing movement. The procedure proceeded with ease once a stable guiding position was secured. IVUS confirmed intra-luminal wire position. The previous stent was undersized at proximal segment. Post-dilatation was done with scoring balloon at high pressure (Scoreflex 3.5x15mm @ 22 atm). Lesion was treated with Drug Coated Balloon 3.5x25mm. LCX was stented uneventfully. Finally IVUS and angiographic results were excellent. Patient was discharged well the next day. 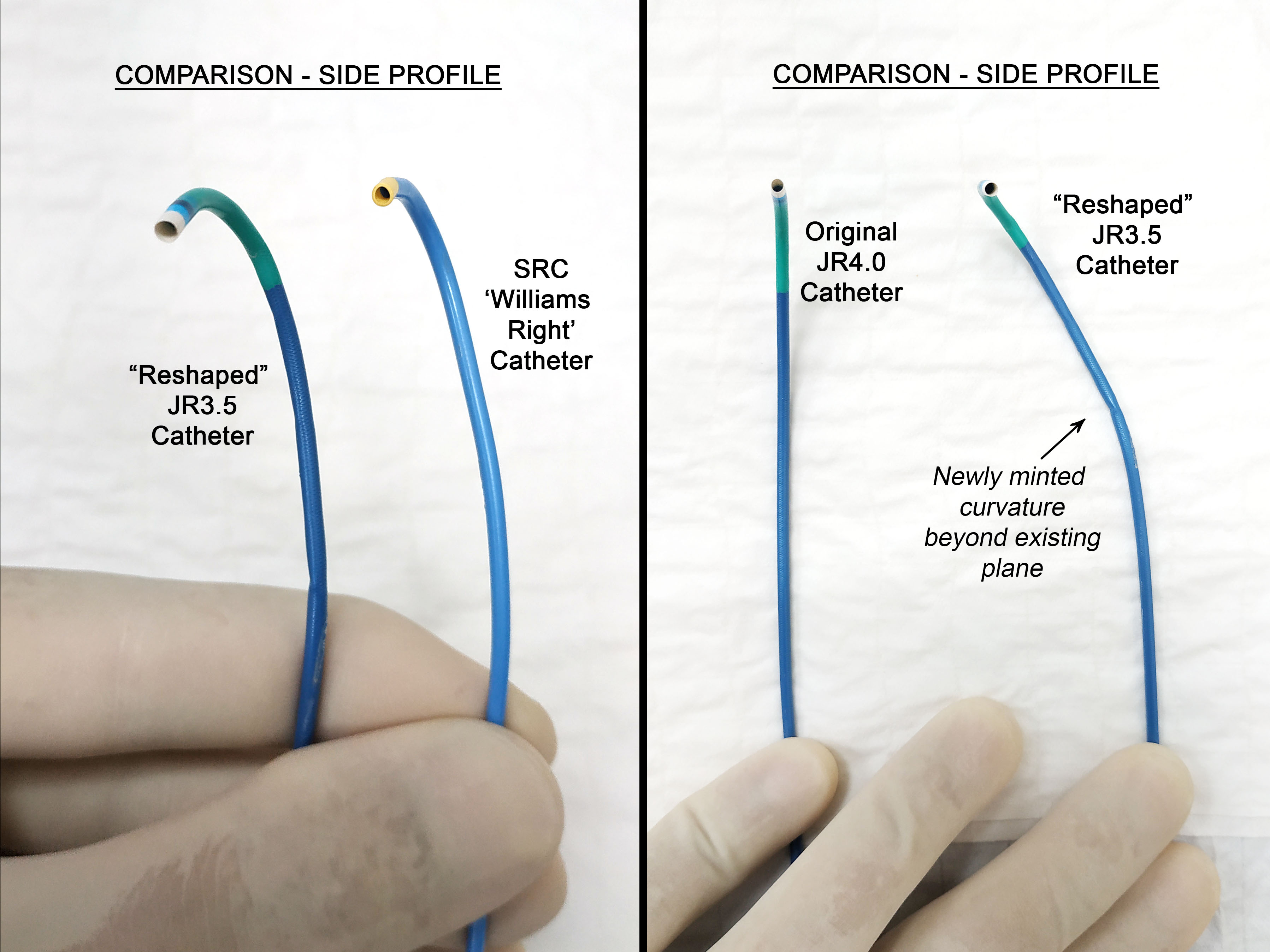 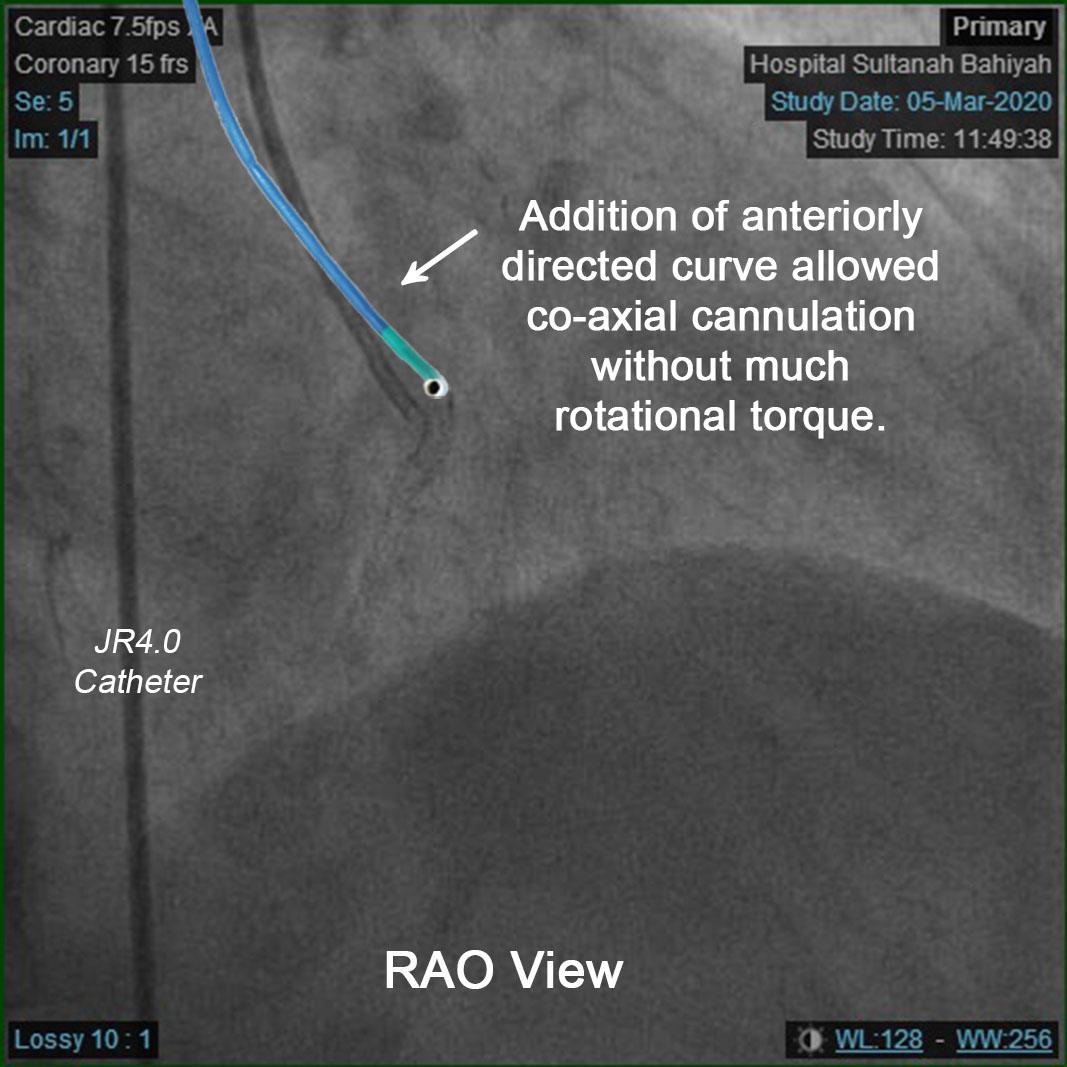 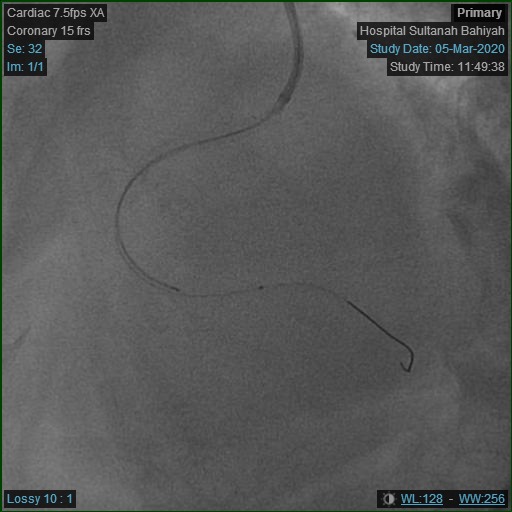 - Case Summary:
PCI remains a highly dynamic and patient-centric procedure. Our case illustrated how meticulous appreciation of structural anatomy and delicate execution could make a difference in challenging yet unconventional situations. However, it should be highlighted that self-modification of any registered products may lead to unforthcoming drawbacks, for instance malformed catheter braiding may lead to damage of traversing devices or entrapment. Thus, extreme precautions must be taken to ensure maximal patient safety beside procedural success.
|
|