Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200408_001
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Acute Myocardial Infarction In A Patient With Secondary Polycythemia | |
| Vicknesan Kulasingham1, Chu Zhen Quek2, Chuey Yan Lee3 | |
| Ministry of Health Malaysia, Malaysia1, Sultanah Aminah Hospital, Malaysia2, Hospital Sultanah Aminah, Malaysia3, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr AJ
-Relevant clinical history and physical exam:
This is a 41 years old man who is an active smoker (10 pack years) presented with sudden onset left sided chest pain at rest. He was previously diagnosed with polycythemia and had venesection done before. On arrival to the Emergency department, he clinically was stable with blood pressure of 157/92 mmHg, HR 62bpm, saturation 98% on air and no clinical signs of failure. His ECG showed ST elevation over inferior leads with right sided involvement. He was given thrombolysis and admitted to CCU.
-Relevant test results prior to catheterization:
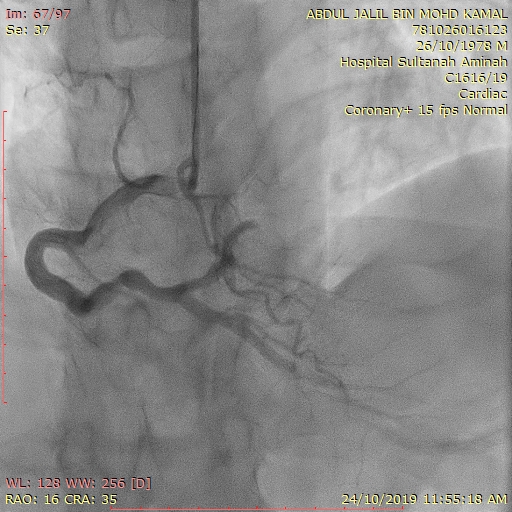
- Relevant catheterization findings:
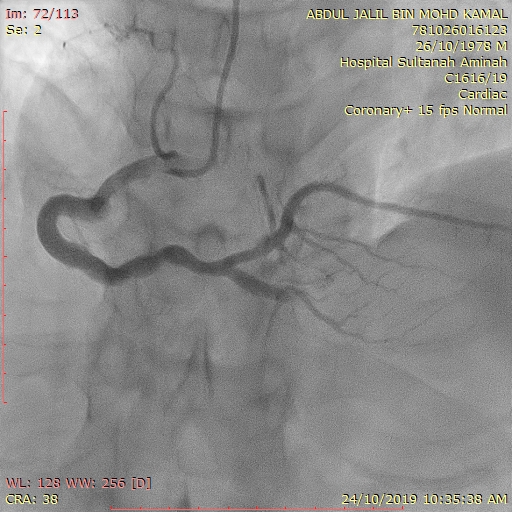
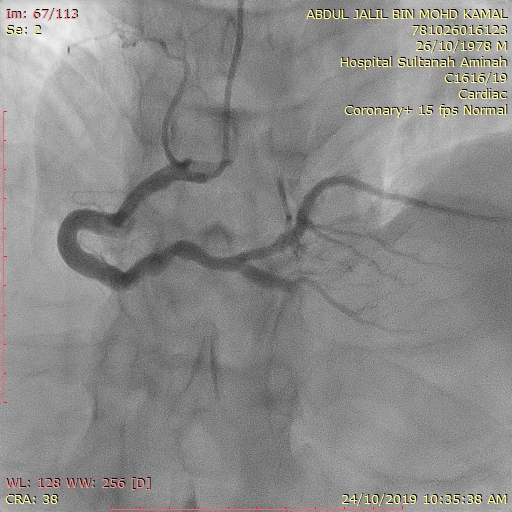
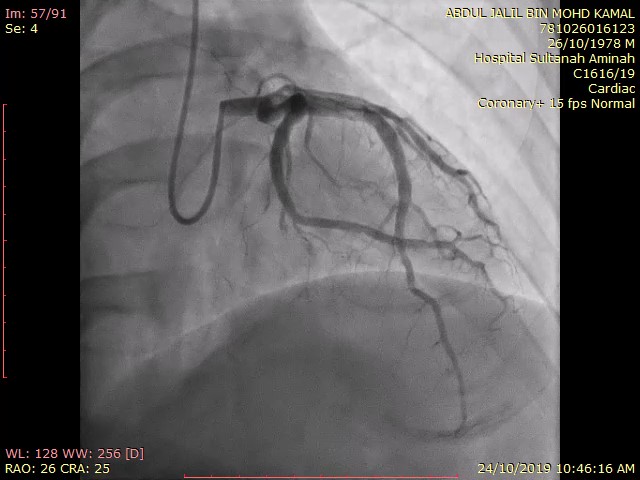
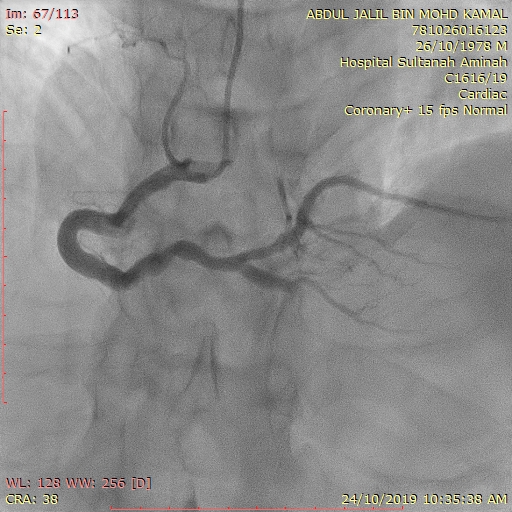
Right radial approach. 6Fr sheath and 5Fr Optitorque diagnostic catheter. Heparin IA 2.5 mg and Heparin IA 7000 units. BP 108/73 mmHg and HR 86bpm. Findings were acute total occlusion of the Posterior Descending Artery(PDA). Other part of RCA and left coronaries was normal
   |
|
|
[Interventional Management]
- Procedural step:
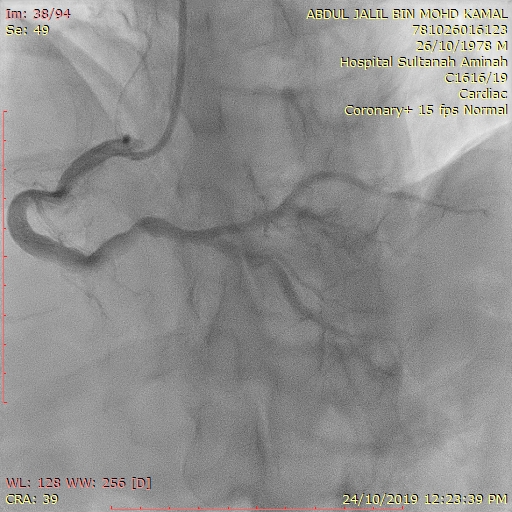
RCA engaged with 6Fr JR4 guiding catheter. Wired to PDA with BMW II. Aspirated with THROMBUSTER and 1 red thrombus aspirated. Subsequently POBA done to PDA using GENOSS 2.5 x 15mm balloon and able to achieve TIMI 3 flow to PDA. IV tirofiban 15 mls given bolus. BMW wire then removed to take final shot. PDA had TIMI 3 flow and had no stenosis seen but noticed that PLV developed acute total occlusion with TIMI 0 flow. ECG showed ST elevation over the inferior leads and patient had chest pain on table. PLV was subsequently wired with the same wire (BMW II). Thrombus aspiration done with THROMBUSTER and 4 large red thrombi aspirated. TIMI 3 flow achieved in PLV and there is no stenosis seen. Screening time 49.2 minutes, total contrast 200 mls and procedure time was 2 hours.
   - Case Summary:
It is well known that any pro thrombotic state predisposes to acute coronary syndrome including acute myocardial infarction. In this case, the patient is polycythemic secondary to heavy smoking which lead him to develop a full blown AMI. His angiogram did not show any stenotic lesion and the occlusion is purely due to thrombus formation in fact developed another AMI during procedure with heavy thrombus load. Post procedure he had a venesection done and was discharged with double anti platelet. Advice was given to stop smoking as well. Further studies may be needed if these patients require anti coagulation since there is no stenosis/atherosclerotic plaque seen.
|
|