Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20200404_001
| CORONARY - Chronic Total Occlusion | |
| Successful Recanalization of Right Coronary Artery Chronic Total Occlusion by Antegrade Dissection and Re-entry Technique Using Stingray Balloon | |
| Kumutha Gobal1, Hou Tee Lu1, Kim Fong Ng1, Doreen Sumpat2, Adelyn Nisha Henry1, Chuey Yan Lee3 | |
| Sultanah Aminah Hospital, Malaysia1, Universiti Malaysia Sabah, Malaysia2, Hospital Sultanah Aminah, Malaysia3, | |
|
[Clinical Information]
- Patient initials or identifier number:
TA
-Relevant clinical history and physical exam:
A 61 years old gentleman, with background history of hypertension, and dyslipidaemia and he is also an active smoker. Presented with Inferior MI in May 2019, was thrombolysed with IV streprokinase as he was undecided for coronary angiogram at that point of time. Subsequently he was seen in the outpatient cardiology clinic and agreed for invasive coronary angiogram. Clinically, he is in CCS class I and NYHA class II. His physical examination was unremarkable
 -Relevant test results prior to catheterization:
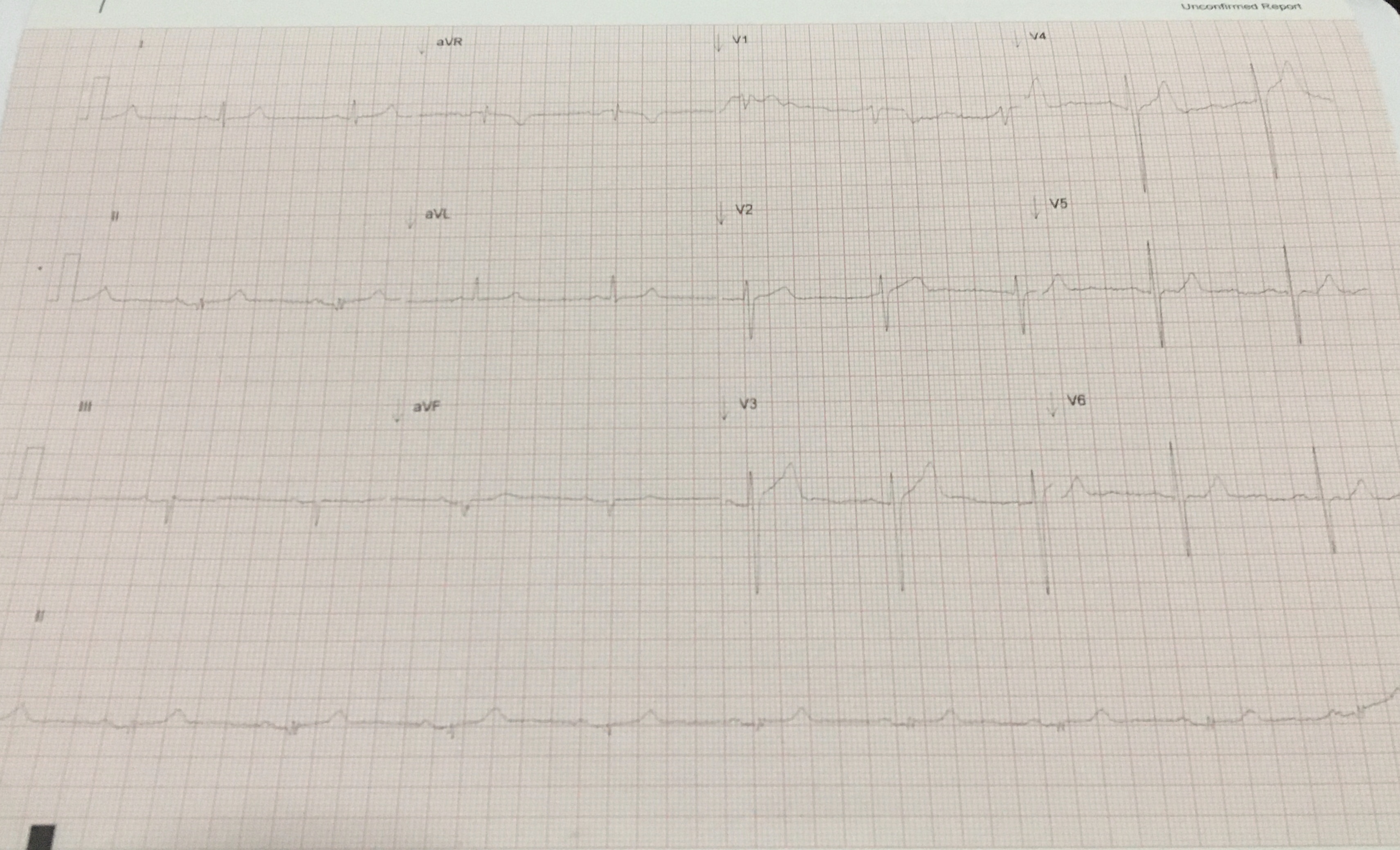
Blood investigations : Hb : 12.9g/dL, creatinine : 85µmol/L, total cholesterol : 4mmol/L, LDL : 2.5mmol/L, RBS : 5.6mmol/l.ECG : sinus rhythm, with no ST changes.Echocardiography showed :VEF of 65-70%, hypokinesia inferoseptal wall. Normal valves and chamber size
- Relevant catheterization findings:
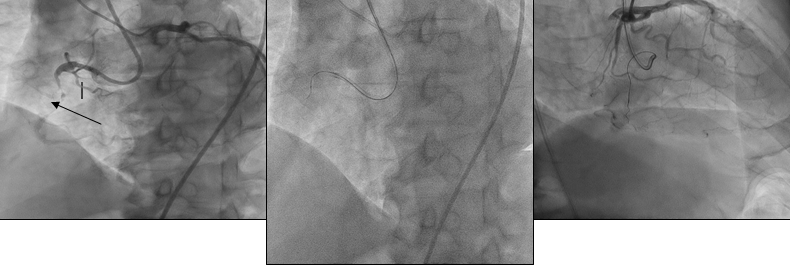
1. Normal left main stem. Normal left anterior descending artery (LAD). Diagonal artery (D1) severe stenosis of 80%. Small septal channel collateral was seen supplying rPDA2. Mid right coronary artery 100% stenosis. (Dominant)3. Normal left circumflex artery (LCx). (Recessive)PCI on CTO was attempted by antegrade approach but unsuccessful. Wire went into sub intimal.Patient was referred for CABG, but patient declined. He was scheduled for second attempt after 2 months
|
|
|
[Interventional Management]
- Procedural step:
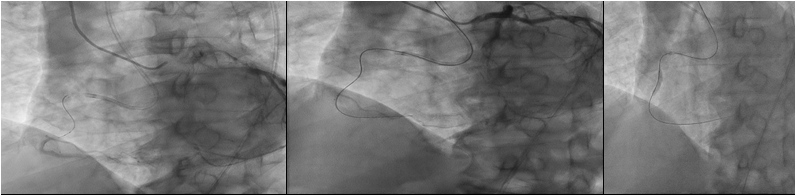
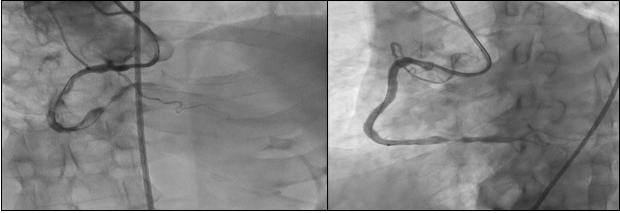
Right radial (6Fr, Optitorque) and femoral arteries (7Fr, AL1) punctured. Initially, trial of AWE (antegrade wireescalation) approach. The RCA CTO was attempted with Fielder XTR wire and Mogul Microcatheter. However, unable to cross lesion, escalated to Cross-IT 100 and200 wire, but wire went into sub intimal. Patientwas well as the septal collateral supplying rPDA was intact. Switched to ADR technique, wire was exchanged with a Hornet 14. Wire was advanced to re-entry zone atmid-distal RCA to facilitate the delivery ofStingray balloon. However delivery of Stingray balloon was difficult. After predilated the sub-intima with 1.0x10mm and 1.5x10mm balloon, the Stingray balloon was positioned at the exit point. Assisted by biplane angiogram with multiple views, the Stingray wire entered thetrue lumen successfully, confirmed by retrograde injection. IVUS showed only a shortsegment of wire was in false lumen. Lesionsfurther predilated with 4.0x15mm balloon. The RCA lesion was stented with DES 4.0x38mm overlapping with 4.0x16mm. Post dilated using NC balloon 5.0x12mm. Post stent implantation IVUS showed the stents were well opposed and expanded with good results.
   - Case Summary:
Antegrade dissection and re-entry technique (ADR) is a good and safe technique to treat chronic total occlusion (CTO) when antegrade wire escalation (AWE) technique failed and lack of suitable intervention collaterals for retrograde approach. Delivery of a stingray balloon into the entry zone can be a challenging matter. A biplane angiogram with multiple views and careful observation could facilitate the correct positioning of the Stingray balloon and re-entry.
|
|