Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191117_001
| CORONARY - Complications | |
| The Long Way for Coronary Angiography via Left Radial Artery Approach: Right Sided Aortic Arch with Aberrant Left Subclavian Artery | |
| Cheng-Hsuan Tsai1, Hsien-Li Kao1, Ying-Hsien Chen1 | |
| National Taiwan University Hospital, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. Lin
-Relevant clinical history and physical exam:
This case is a 76-year-old man with hypertension, diabetes mellitus and dyslipidemia. He smoked 1 pack a day for up to 30 years. He presented with progressive chest tightness with intermittent cold sweating for 2 months before the index procedure.
-Relevant test results prior to catheterization:
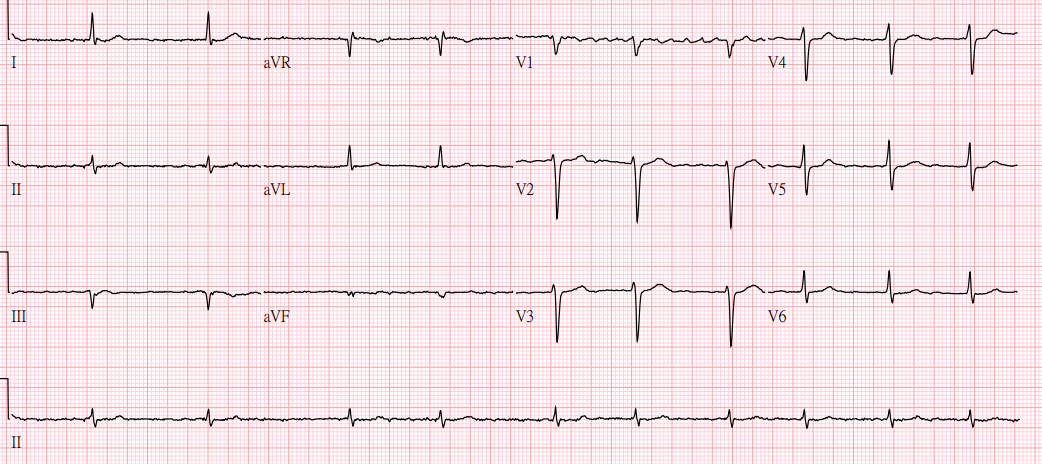
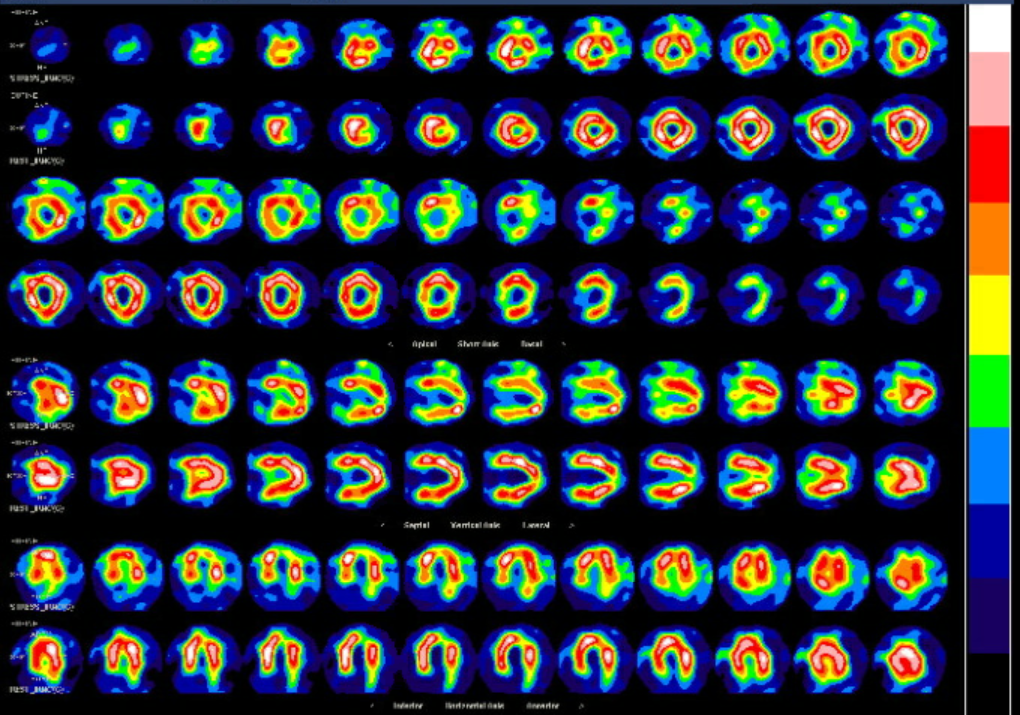
The electrocardiogram showed atrial fibrillation rhythm and small inferior leads Q waves. Chest X-ray showed tortuosity of aorta and cardiomegaly. Thallium 201 myocardial perfusion scan revealed reversible perfusion defect at anterolateral and inferior region.
   - Relevant catheterization findings:
Left coronary angiography showed mild stenosis in first diagonal branch and small obtuse marginal branches. Right coronary angiography showed proximal portion 80%stenosis and distal portion 90% stenosis which extending to proximal PDA.
|
|
|
[Interventional Management]
- Procedural step:
The coronary angiography was performed via left radial artery approach. However, it was difficult to passed the Terumo wire to ascending aorta. The aortography demonstrated the unusual location of descending aorta. The diagnosis of right sided aortic arch with aberrant left subclavian artery was suspected. After manipulating the Terumo wire through the aortic arch and to the ascending aorta, we can deliver the left Judkins catheter and right Judkins catheter for selective angiography. The percutaneous coronary intervention (PCI) for right coronary artery stenosis is indicated. However, PCI through left radial artery was almost impossible due to extreme tortuous route. Therefore, right femoral artery approach was selected for PCI. The course of aorta was demonstrated by 0.035 inches wire before intervention. A 6F AL1 guide catheter was engaged to RCA orifice. Sion was wired to distal PDA followed by sequential balloon dilatation. A 3x22 Resolute Onyx drug-eluting stent was placed on proximal portion of RCA. In addition, prolong balloon dilatation with 2.5x3 Agent drug-coating balloon was performed to distal portion of RCA. The procedure succeeded without complication. The reconstruction CT angiogram of aorta after the index procedure also confirmed the diagnosis of right sided aortic arch with aberrant left subclavian artery.
 - Case Summary:
The right-sided aortic arch is a rare anatomical variant present in about 0.1% of the adult population. It is classified into three types. In type 1, the major arteries branching out from the arch and in type 2, an aberrant left subclavian artery originated from descending aorta like this case. The type 3, left subclavian artery is isolated and does not attach to the aorta. For interventional cardiologists, aware this diagnosis is critical during PCI. Femoral artery or right radial artery approach is the better choice for cardiac catheterization in these patients, especially those with type 2 and 3 right-sided aortic arch.
|
|