Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191116_003
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| OCT Guided PCI of Proximal LAD ISR in NSTEMI: Seek the Truth and See the Truth to Believe It | |
| Harish Oruganti1 | |
| Kims, India1, | |
|
[Clinical Information]
- Patient initials or identifier number:
SR
-Relevant clinical history and physical exam:
A 50-year-old female patient presented with typical chest pain since 3 days. On evaluation her BP was 140/90 mm Hg and on auscultation basal crepitations were heard in both lungs. Heart sounds were normal. she has a past history of coronary artery disease details for which she underwent PCI of proximal LAD 2 years back and was on regular medication of aspirin and rosuvastatin since then.
-Relevant test results prior to catheterization:
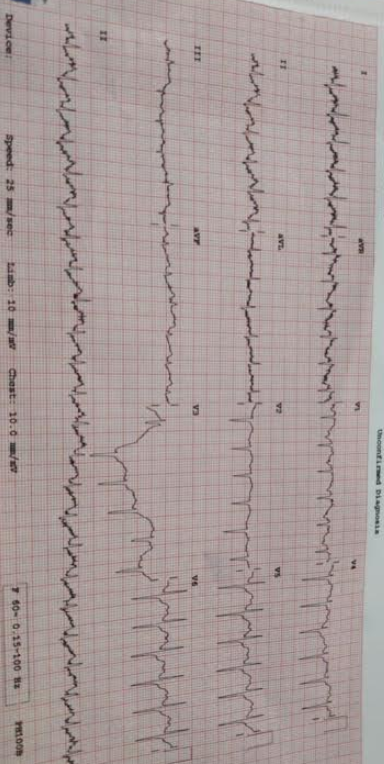
ECG showed ST elevations in avR and v1 and ST depressions in other precordial leads. with sinus tachycardia. Echo showed RWMA in anterior territory with moderate LV dysfunctions and mild mitral regurgitation.
 - Relevant catheterization findings:
coronary angiogram was done which showed significant in-stent restenosis of proximal LAD stent, LCX and RCA were normal and therefore PCI was planned for image guided PCI of LAD
|
|
|
[Interventional Management]
- Procedural step:
Right femoral access was chosen and EBU 3.5 X 6 Fr guide catheter was used to engage Left coronary artery and preprocedural OCT pullback imaging was with 15 ml of contrast injection. PCI was done by sequentially predilating the stented portion with 2mm and 2.5mm diameter non-compliant balloons. Stent size was chosen according to the vessel dimensions observed in the OCT run. 3X28mm XIENCE V stent was deployed at 12 atmospheres and post dilated with 3.5 mm non-compliant balloon up to 16 atmospheres. Angiographic result was good with TIMI 3 flow. Final result was confirmed with repeat OCT pullback imaging to assess the stent apposition, Expansion and edge dissections if any. OCT imaging showed perfect apposition of deployed stent with no edge dissections.
- Case Summary:
Angiography may give false impression of stent apposition in few cases as has been noted in many studies compared with intracoronary imaging. The ease of interpretation and accuracy of finding makes OCT a better choice in this scenario. We have chosen OCT guided PCI in this patient as we wanted to know the reason for in-stent restenosis in this patient and it was found to be malapposition. OCT imaging helped us in achieving good approximation of stent in this patient. Seek the truth and see the truth to believe it.
|
|