Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191116_002
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Jailed Balloon Technique for Provisional Stenting Approach to Coronary Bifurcation Lesion with Intravascular Ultrasound Evaluation: The First Case Experience at Hua Hin Hospital | |
| Polpat Euswas1 | |
| Hua Hin Hospital, Thailand1, | |
|
[Clinical Information]
- Patient initials or identifier number:
JB-001
-Relevant clinical history and physical exam:
71-year-old male with hypertension, dyslipidemia.He was presented with progressive dyspnea on exertion with positive exercise stress test and referred for coronary angiogram.There were no sign of congestive heart failure and neurological deficit.
-Relevant test results prior to catheterization:
Baseline ECG was shown normal sinus without significant ST-T abnormality.Echocardiogram were shown LVEF 59 % without wall motion abnormality. No significant valvular lesion.Coronary angiogram was performed.
- Relevant catheterization findings:
Diagnosis was triple vessels disease. Left main coronary artery was no stenosis. Left anterior descending artery was 30 % stenosis at ostial part, 95 % stenosis at proximal part and ostial DG1 (Medina 1-1-1) with tubular change at proximal DG1. Left circumflex artery was 99 % stenosis at mid LCX (small caliber). Right coronary artery was 90 % stenosis at distal right posterolateral branch.
|
|
|
[Interventional Management]
- Procedural step:
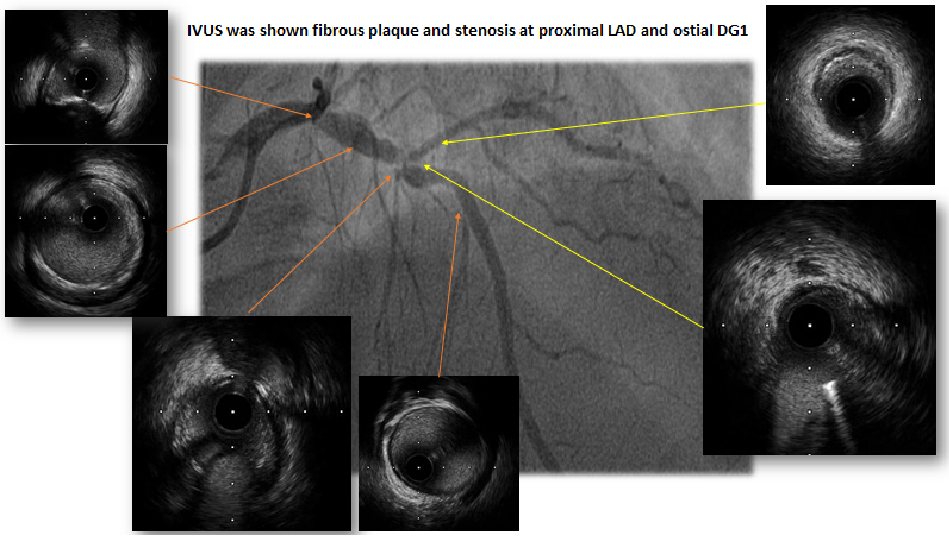
PCI at LAD/DG1 was start with right femoral artery access. Guiding catheter was JL 3.5, 7 French. Guide wire were to LAD and DG1. Intravascular ultrasound was checked at LAD and DG1. IVUS was shown fibrous plaque and stenosis at proximal LAD and ostial DG1. Jailed balloon technique was performed. Pre-dilatation with non-compliant balloon 3.5 / 15 mm. 3 atm. at proximal LAD. Cine after pre-dilatation at proximal LAD. Stenosis at ostial DG1 was observed. Drug-eluting stent 3.0 / 24 mm. to proximal LAD. semi-compliant balloon 2.0 / 20 mm. to DG1. Pre-dilatation at DG1 semi-compliant balloon 2.0 / 20 mm. 8-10 atm. Make position of Semi-compliant balloon DG1 (2.0 / 20 mm.) proximal dot at proximal stent part. Then inflated stent 3.0 / 24 mm, 10 atm. .Next, inflated both (stent balloon at LAD and DG1 balloon), 12 atm (used 1 in-deflator with special 3-way connection). DG1 balloon was removed, then re-inflated stent balloon at proximal LAD. Post-dilatation with non-compliant balloon 3.5 / 15 mm, 4-6-12-14 atm. IVUS at LAD after PCI with NC balloon post-dilatation. After post-dilatation Cine was shown good flow at LAD and DG1 with some stenosis at ostial DG1. IVUS was shown good stent expansion and apposition, no dissection.
 - Case Summary:
Coronary bifurcation lesions comprise roughly 15 – 20 % of PCI. Side branch occlusion after main branch stenting occurs in 7.4 – 8.4 % of bifurcation lesion and brings with a serious complication during PCI. In practice, significant side branch is a branch that the operator does not want to lose after evaluating the individual patient. Jailed-Balloon Technique is a technique aimed at improving side branch protection during provisional stenting of bifurcated lesions considered at high risk of side branch compromise after main vessel stenting, associate with high procedural success rate, improved side branch patency and low immediate cardiac event rate.
|
|