Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191116_001
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| OCT Guided PCI with Stenting of ISR of Ostial LAD | |
| Kala Jeethender Kumar1 | |
| Yashoda Hospitals Hi-Tech City, India1, | |
|
[Clinical Information]
- Patient initials or identifier number:
RR
-Relevant clinical history and physical exam:
55 years old male known hypertensive and diabetic presented with chest pain associated with shortness of breath. Post PCI of LAD (3.0x18mm BioMime stent) in 2018, On Examination PR-70/min, Bp-110/80mmHg, SPO2-98%, Heart-S1+,S2+,S30,S40, Investigations-Hb-12gms%, RBS-151g/dl, S.Cr-0.7mg/dl,B.Urea-42mg/dl, HBsAg, HCV, HIV-I&II-Negative, Serum electrolytes-normal, BloodUrea-18mg/dl,
-Relevant test results prior to catheterization:
ECG-NTEMI, 2D Echo-No RWMA, normal LV function, EF-60%.
- Relevant catheterization findings:
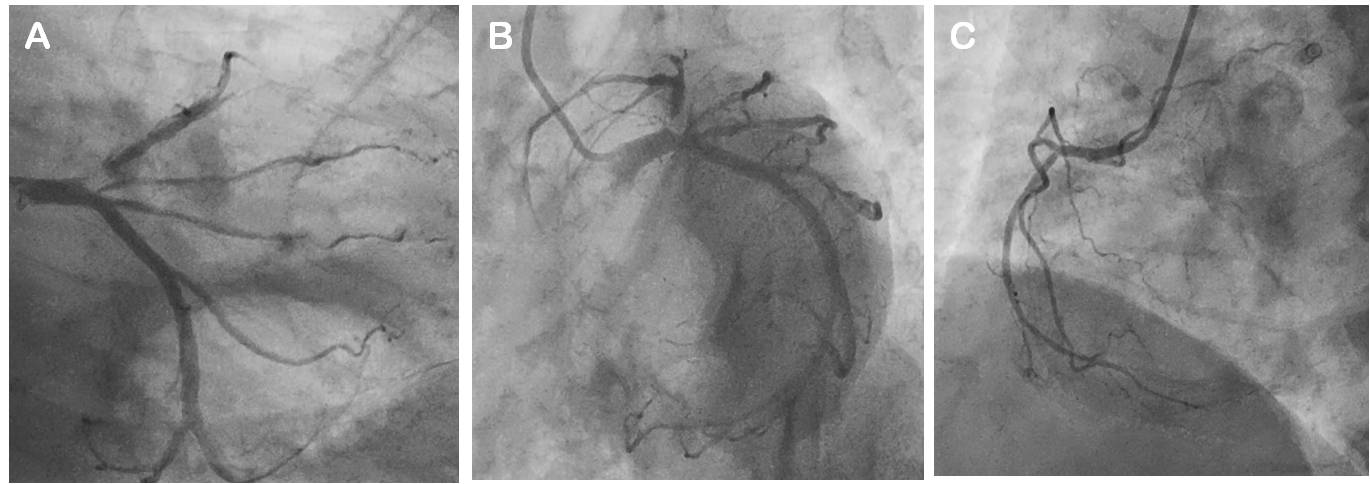
Coronary angiogram showed single vessel disease, LMCA-Normal, LAD-ostial LAD in-stent resteosis with TIMI-I flow, LCX-Normal, RCA-Normal.
 |
|
|
[Interventional Management]
- Procedural step:
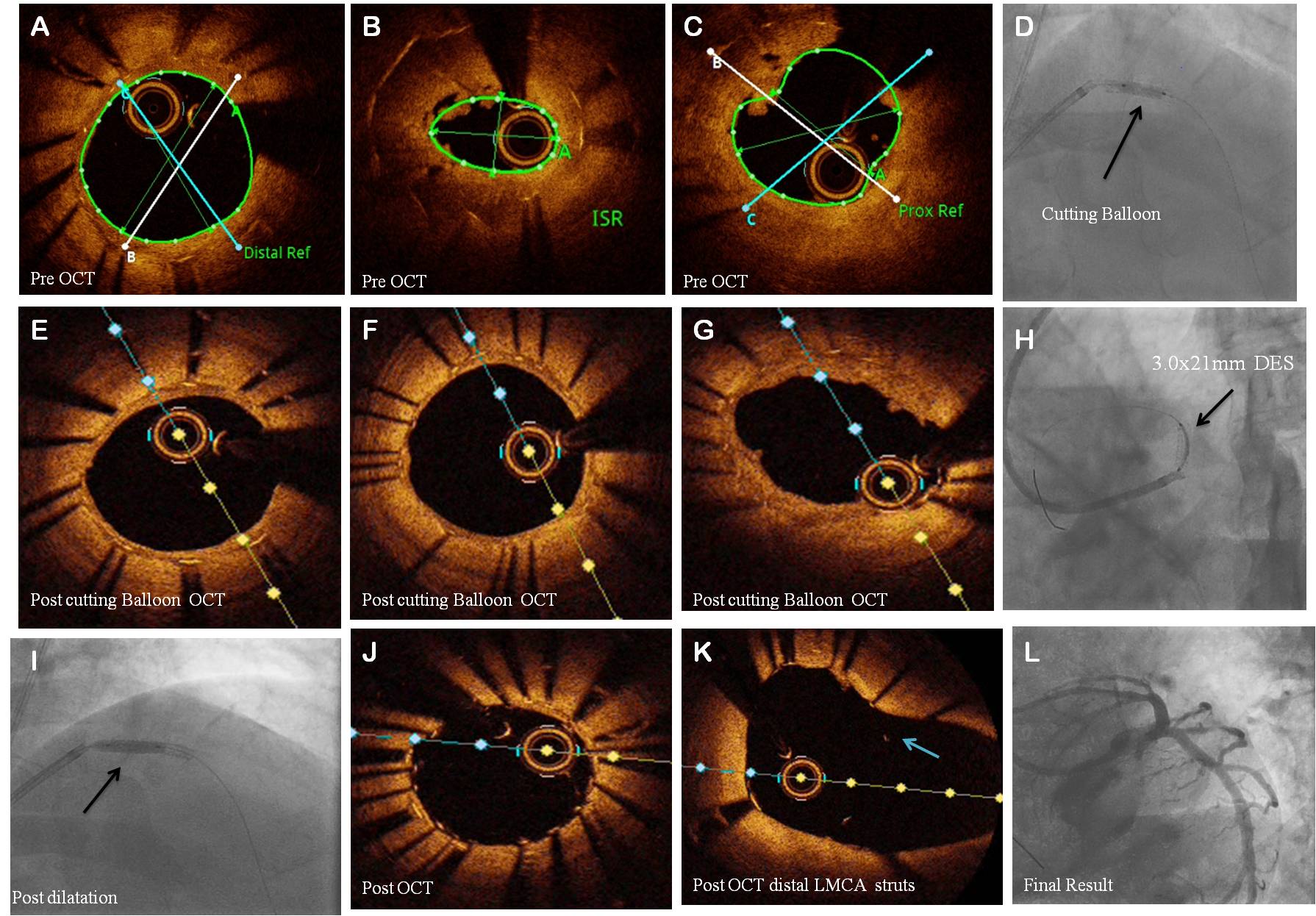
Procedure performed through right femoral artery using 7Fr EBU 3.5 Guiding catheter, Check angiogram revealed ostial LAD ISR. 0.014"Sion blue wire crossed the lesion. Predilatation done with 1.0x10mm Sapphire, 1.5x10mm Tazuna, 2.0x12mm Trek and 2.5x15mm NC Trek Balloons. Pre procedure OCT showed ISR of ostial LAD with MLA 1.48mm2, MLD 1.35mm, distal landing zone MLA 5.00mm2, MLD 2.52mm, proximal landing zone MLA 3.59mm2, MLD 2.13mm and length of the lesion 20mm. Predilatation done with 2.5x12mm cutting balloon. Post cutting balloon OCT study showed distal portion of the lesion with MLA 3.96mm2, mid portion of the lesion with 3.12mm2, and proximal portion of the lesion with MLA 3.25mm2. Ostial LAD stenting done with 3.0x21mm Xience prime stent (DES). Postdilatation done with 3.0x10mm NC Trek Balloon. Post OCT study showed stent struts in distal LMCA, well-apposed stent struts with MLA 4.86mm2, no residual stenosis, no edge dissection and. Post procedure AngioView showed well implanted stents with TIMI-III flow without any dissection. Patient was discharged on 3rd post procedure in a stable status.
 - Case Summary:
OCT very helpful tool for identifying abnormalities related to the stent and underlying vessel wall which have been associated with risk of stent thrombosis like edge dissection, malapposition, geographic plaque miss, and tissue prolapse. OCT is more accurate and sensitive for visualizing subtle stent—or lumen—related morphologies and OCT especiailly very useful in distal left main and ostial LAD lesions when instent restenosis is there. OCT used for optimization of PCI.
|
|