Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191115_032
| CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP) | |
| Rotablate the Vessel of a Fragile Old Lady | |
| Shihjung Jang1 | |
| Buddhist Taipei Tzu Chi hospital, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mrs. Lin
-Relevant clinical history and physical exam:
This 89-year-old female is a dialysis patient with diabetes and hypertension. She had been admitted in this late April for acute non-ST elevation myocardial infarction with the initial presentation as chest tightness and elevating high sensitivity troponin-I level (614 ng/L). Coronary angiogram showed calcified vessels with left main and triple vessel diseases. Because of recent lower gastrointestinal bleeding with sigmoid colon tumor, medical treatment was advised.
-Relevant test results prior to catheterization:
The patient and family declined bypass surgery after surgeon evaluation (STS risk score of mortality was 9.184%). At outpatient visit, clopidogrel was treated under subsided gastrointestinal bleeding. The patient had recurrent angina and another episode of acute non-ST elevation myocardial infarction developed in this July with higher high sensitivity troponin-I level (5950.3 ng/L). Due to refractory angina, the family requested percutaneous coronary intervention including atherectomy.
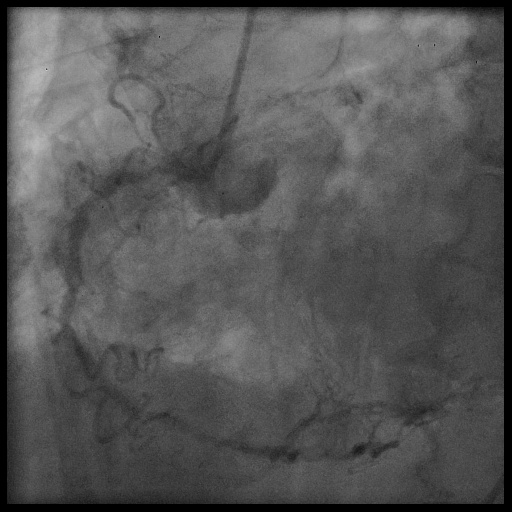
- Relevant catheterization findings:
Coronary angiogram in August revealed diffusely calcified vessels with left main and triple vessels. Critical left anterior descending artery lesions and progressed right coronary artery lesion were found.
   |
|
|
[Interventional Management]
- Procedural step:
Scheduled intervention started with right groin approach. Left femoral artery puncture was prepared for backup access. 7 French BL 3.5 guiding catheter was used with Asahi Fielder XT-R wire. We needed to dilated the tight LAD lesions by Kaneka Ikazuchi balloon 1.0 * 6 mm. A Vascular solutions Turnpike Gold catheter further dilated the lumen before Terumo Finecross microcatheter was inserted to exchange Rota floppy wire. Hypotension developed then. Vasopressor infusion and intra-aortic balloon counterpulsation were supported. Right femoral vein was punctured for pacing wire access. Under stabilized hemodynamic status, the Boston Scientific Rotalink Plus 1.50mm (0.059in) burr was used for rotational atherectomy of LM to LAD middle segment. Totally 5 sessions with 150,000-180,000rpm speed were performed (< 15 seconds per session). Left circumflex artery slow flow was found before rotablation. Asahi Sion Blue ES wire was exchanged for better support before further balloon dilatation. LM to LAD distal segment was dilated by Terumo Tazuna 2.5 * 10 mm balloon and Medtronic NC Euphora 3.0 * 15 mm balloon. A Boston Scientific Synergy drug eluting stent (2.5 * 48 mm) was placed at LAD middle to distal segment. LCX lesions were treated by balloon angioplasty and stenting with Synergy stents 3.0 * 16 mm plus 3.0 * 12 mm. Final stenting of LM to LAD proximal segment was performed with a Synergy stent 3.5 * 38 mm. Intra-vascular ultrasound evaluation was performed during the procedure.
- Case Summary:
For high risk patient, percutaneous coronary intervention with rotational atherectomy could be feasible under careful planning. Moreover, hemodynamic support including mechanical device should be prepared for any unstable event.
|
|