Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191115_028
| CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP) | |
| Management for Calcified Ostial Left Main and LAD Lesions | |
| Tsung Han Lin1, Chun-Yuan Chu2 | |
| Kaohsiung Municipal Ta-Tung Hospital, Taiwan1, Kaohsiung Medical University Hospital, Taiwan2, | |
|
[Clinical Information]
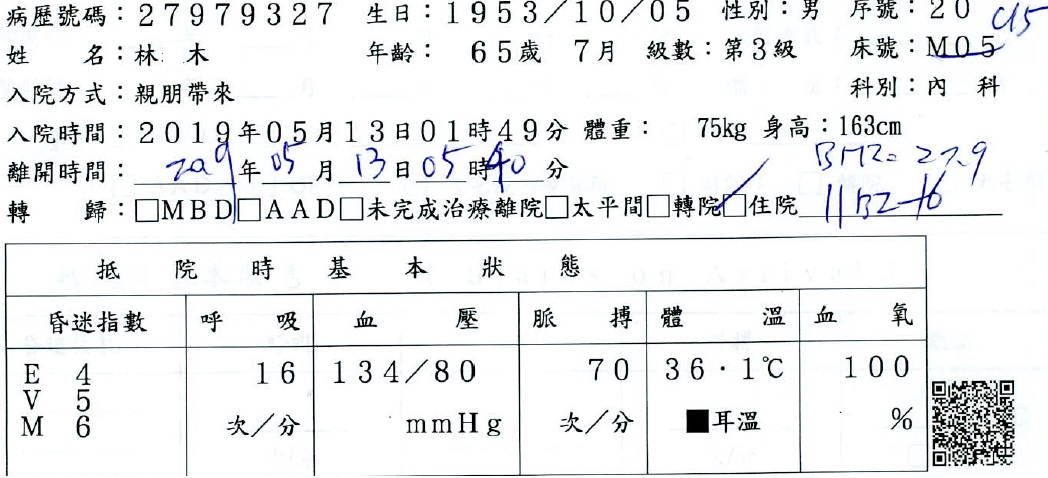
- Patient initials or identifier number:
Mr. Lin, Chart number 27979327
-Relevant clinical history and physical exam:
This case is a 65-year-old man. He had underlying disease of type 2 diabetes mellitus and end stage renal disease, both had regular follow up at Outpatient Department. Initial presentation was intermittent typical chest pain for one week. He came to our Emergency Department on 2019/5/13. Initial vital signs at our Emergency Department revealed blood pressure: 134/80mmHg, body temperature: 36.1’C, heart rate: 70bpm, respiratory rate: 16rpm.
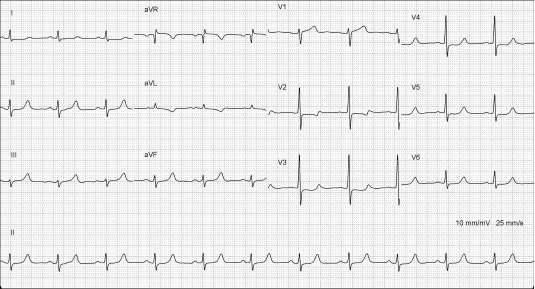
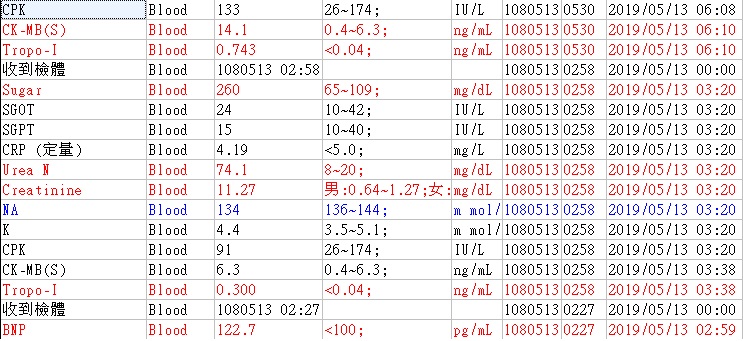
 -Relevant test results prior to catheterization:
Laboratory data showed elevated cardiac enzymes and electrocardiogram showed general precordial lead ST segment depression. Non-ST-segment elevation myocardial infarction was diagnosed therefore dual-antiplatelet were given and heparinization was done.
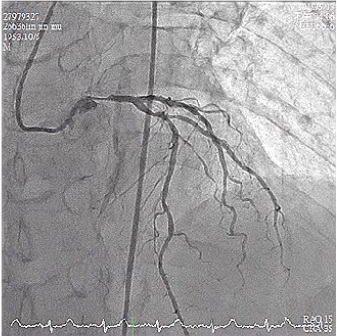
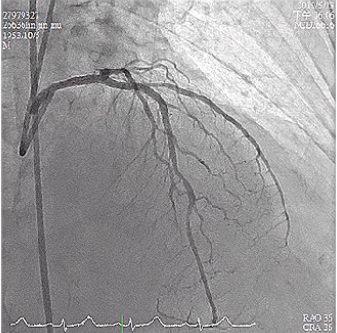
  - Relevant catheterization findings:
Coronary angiography was performed which reported left main artery proximal 90% stenosis, right coronary artery nonsignificant stenosis, left anterior descending artery proximal 80% stenosis and left circumflex artery no significant stenosis.
  |
|
|
[Interventional Management]
- Procedural step:
Percutaneous coronary intervention for left main to left anterior descending artery was performed. We used EBU 3.5 7F as guiding catheter and Runthrough Hypercoat as guide wire then advanced to left anterior descending artery. Intravascular ultrasound (IVUS) showed heavy calcified stenosis since left anterior descending artery to proximal left main artery. Then we changed Runthrough Hypercoat to Rota wire, started rotablation with 1.5mm burr 160000rpm from left main artery to middle left anterior descending artery. Plain old balloon angioplasty with 2.5x15 mm NC Emerge balloon dilated at left anterior descending artery with maximum 24 atm and 3.0x20 mm AccuForce balloon dilated at left main to left anterior descending artery with maximum 16 atm, then 3.0x34mm Onyx stent was deployed at left anterior descending artery with 10atm and 3.5x28mm Xience stent was deployed at left main to left anterior descending artery with 12 atm. Post-dilatation was done with AccuForce 3.0x20 mm dilated up maximum 20 atm and NC Euphora 4.0x8 mm dilated up maximum 24 atm.
 - Case Summary:
The coronary angiography on my case showed severe calcified in left main artery and left anterior descending artery ostium. It may have caused stent malposition if used plain old balloon angioplasty and stenting over the lesion after POBA. Rotational atherectomy may be considered to manage the severe calcified lesion, then followed POBA and stenting. Final angiography showed TIMI 3 flow on this case.
|
|