Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191115_019
| CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP) | |
| Complete Revascularization Under Support of ECMO | |
| I-Fan Liu1, Tien Ping Tsao1 | |
| Cheng Hsin General Hospital, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
H.T.W
-Relevant clinical history and physical exam:
This 83-year-old male is a patient with CAD with LM and 3VD s/p CABG X 4 (LAD, LCX-P,PL-PDA) 1 year prior to this admission. He complained of dyspnea on exertion, chest tightness, leg edema, dizziness, abdominal fullness and weakness for 2-3 months. CXR showed bilateral pleural effusion. He was admitted for decompensated heart failure. The echo showed that LVEF was 23%. He also reported chest tightness. Coronary angiography was done.
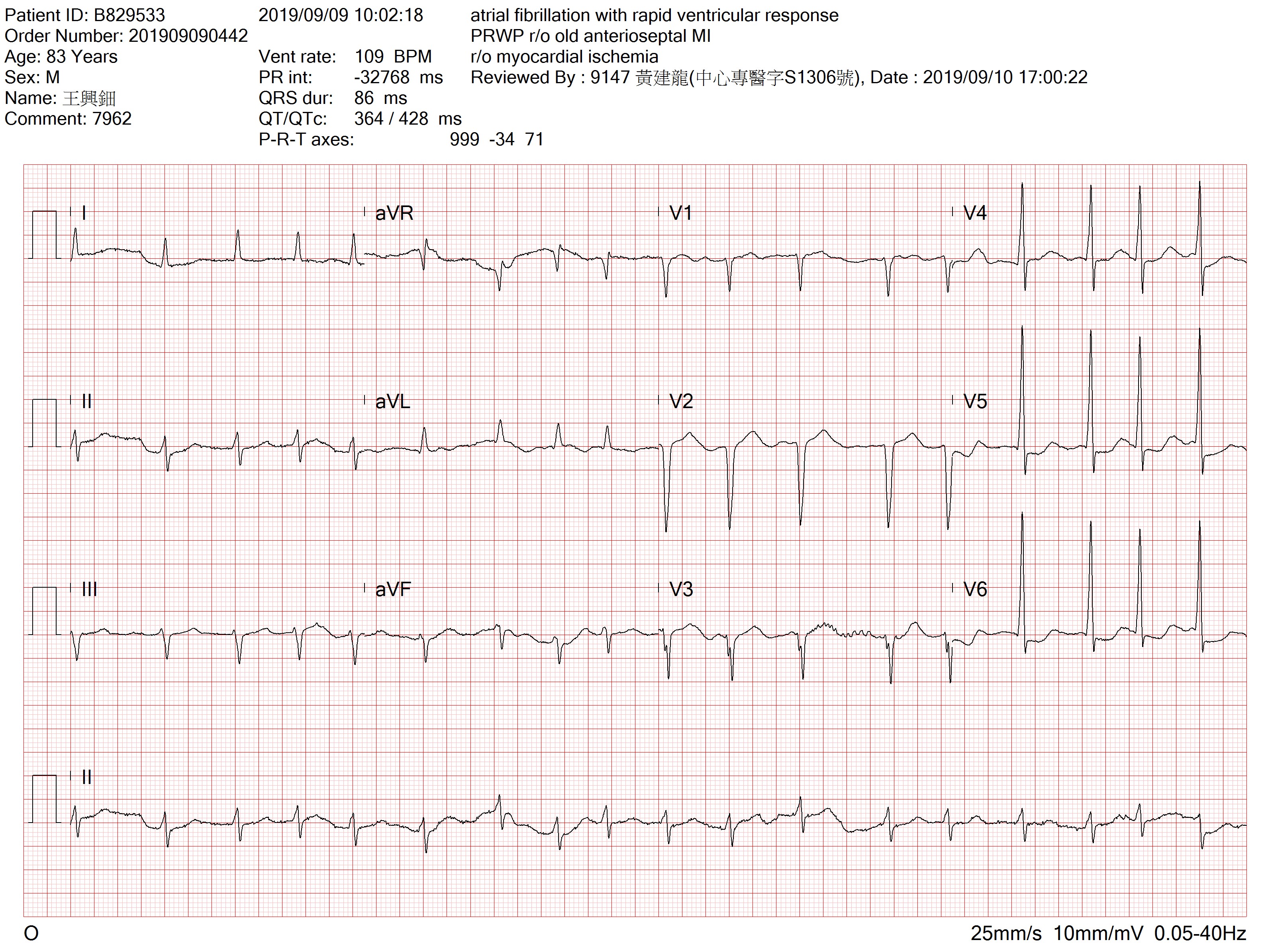
-Relevant test results prior to catheterization:
The EKG showed atrial fibrillation and old anterior wall MI. The echocardiogram showed that LVEF was 23% and severe MR and TR.
 - Relevant catheterization findings:
1.LM- D/3 eccentric 80% narrowing. 2.LAD- P-M/3 area CTO, competitive flow. 3.LCX- Luminal changes, no retrograde flow. 4.RCA- PDA tandem lesions: near total. SVGs to LAD and LCx were not visualized. SVG to RCA was patent.
|
|
|
[Interventional Management]
- Procedural step:
ECMO was implanted before PCI. LMCA was engaged with an EBU 3.5 7F with side holes. A 3.5x15 mm balloon dilated LM-LCx. A Crusade catheter to assist LM-LAD wiring but failed. Another Pilot 50 wire was used for reversed wire but failed. Selected a Fielder FC wire for reversed wire technique, and it entered LAD and could be advanced to DB1. A Finecross microcatheter was advanced to proximal LAD and removed Fileder FC and a Runthrough wire could cross the nearly occluded and calcified mid-LAD and was advanced to distal LAD. A 2.0 x 20 mm balloon dilated the mid-LAD. IVUS checked LM-LCx and some plaque was noted at proximal LCx, the vessel diameter was 4-4.5 mm in proximal LCx and 5 mm in LM. IVUS also checked LAD and calcification over mid-LAD with vessel diameter 2.5-3.0 mm noted. A 2.25 x 15 mm NC balloon dilated the mid-LAD. A 2.25 x 22 mm DES was deployed. Post dilated with a 2.5 x 12 mm NC balloon. A 4.0 x 22 mm DES was deployed at LM-LCx with minimal protrusion into LM at 16 atm. Rewired LM-LAD with a Pilot 50 wire and removed the jailed Runthrough wire. A 4.5 x 12 mm NC balloon post dilated the LM at 18 atm as POT. IVUS LM-LCx showed good stent expansion and stent apposition. A Pilot 50 wire was advanced to distal PL batch. A 3.5 x 15 mm balloon dilated the lesion. A 3.5 x 23mm DES was attempted to insert into the lesion but failed due to angulation of mid-RCA. A Guidezilla catheter was advanced to close the lesion site. and was deployed. ECMO was removed after PCI.
- Case Summary:
PCI for CHIP patient is challenging. For post-CABG patients, complex PCI is usually the only revascularization option. Proper use of mechanical circulatory support is one of most important factors of success of the high-risk procedure.
|
|