Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191115_007
| CORONARY - Complications | |
| Catheter-induced Iatrogenic Right Coronary Artery Extensive Dissection Successfully Treated with IVUS-Guided PCI | |
| Towong Jirotjananukul1, Sukhum Tachasakunjaroen2, Krissada Meemook3 | |
| Mahidolbumrungrak, Thailand1, Police General Hospital, Thailand2, Ramathibodi Hospital Mahidol University, Thailand3, | |
|
[Clinical Information]
- Patient initials or identifier number:
4557643
-Relevant clinical history and physical exam:
A 47-year-old ex-smoker male was admitted for elective coronary angiogram due to history of NSTE-ACS about 2 months ago. He has a past medical history of hypertension, dyslipidemia and ESRD S/P LRKT. His physical examination was unremarkable.
-Relevant test results prior to catheterization:
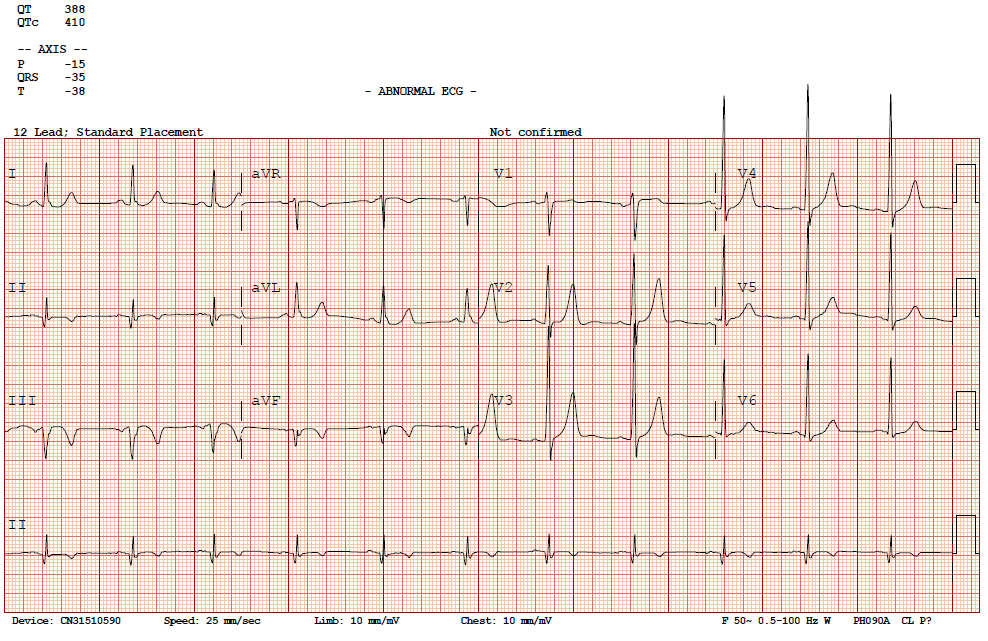
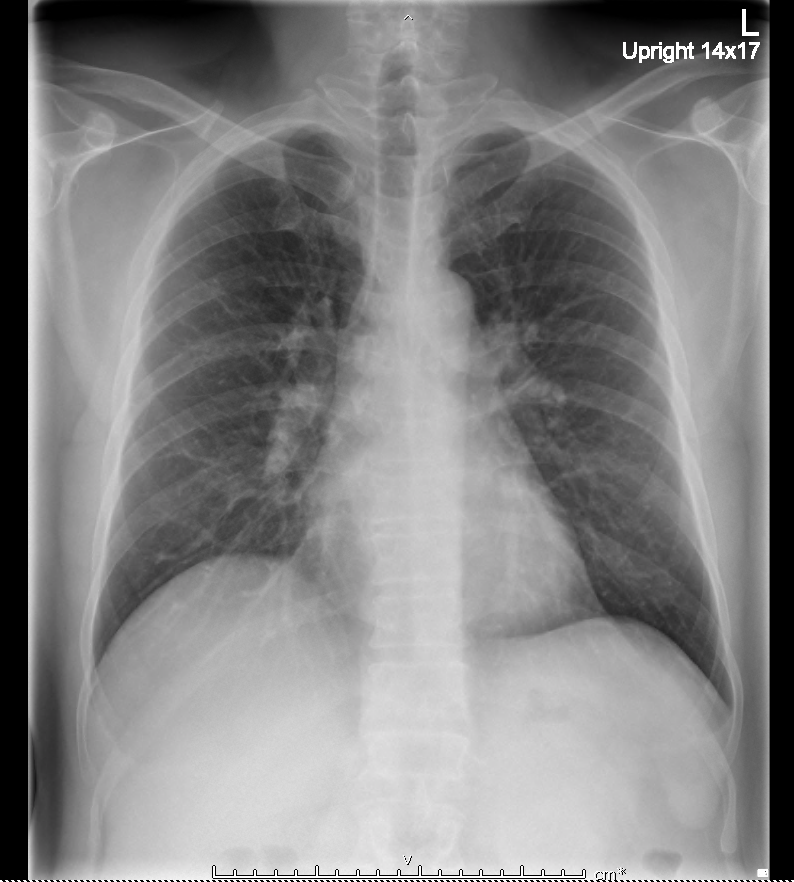
The simple chest radiography was unremarkable. His baseline ECG showed sinus rhythm with Q wave and T wave inversion at II, III and aVF. His echocardiogram showed mildly impaired LV systolic function (LVEF 50%) with hypokinesia at inferior wall.
  - Relevant catheterization findings:
1. 1. The right coronary angiogram showed severe diffuse stenosis from proximal to distal RCA.2. 2. The left coronary angiogram showed severe tubular stenosis of DG2, distal LAD and proximal LCx.
|
|
|
[Interventional Management]
- Procedural step:
A 6F sheath was inserted through right radial artery, and the right coronary ostium was engaged with a 6F GUIDING AL1 short tip catheter. A 0.014-inch 180 cm FIELDER FC wire was inserted into RCA. The RCA was sequentially pre-dilated by MOZEC balloon 1.5 x 15 mm and CONQUEROR balloon 2.5 x 20 mm. Following coronary angiogram revealed RCA dissection. The guide wire was accidentally disengaged due to difficult to manipulation. 6F GUIDING JR 3.5 100 cm and 0.014-inch 180 cm RUNTHROUGH wire were successfully re-engaged to RCA. The following IVUS ensured true lumen wiring and showed extensive spiral dissection of RCA. We decided to deployed 4.0 x 33 mm FIREBIRD II at proximal RCA for cover dissection plane. Pre-dilatation at distal RCA by CONQUEROR balloon 2.5 x 20 mm followed by FIREBIRD II DES 2.5 x 33 mm deployment at distal RCA. Then, two FIREBIRDE II DES 3.0 x 33 mm and 3.5 x 33 mm were deployed at mid to distal segment. Post-dilatation were performed with FORTIS balloon 3.5 x 18 mm and balloon stent 4.0 x 33 mm. The final angiogram and IVUS examination showed good results.
- Case Summary:
Catheter-induced iatrogenic coronary artery dissection is a rare condition but potentially fatal complication. Many risk factors are described such as LM disease, catheterization for ACS, predisposing arteropathies and using of Amplatz-shaped catheter. Careful guiding catheter manipulation is mandatory. However, if it occurred, securing and maintaining wire access across the dissected artery is the most important consideration.
|
|