Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191115_006
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Myocardial Bridge in ST Elevation Myocardial Infarction: The Crux of the Matter | |
| Hendy Bhaskara Perdana Putra1, Benny Jovie1, Ragil Nur Rosyadi1, Quri Meihaerani Savitri1 | |
| Dr. Ramelan Navy Hospital Surabaya, Indonesia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
11.87.13
-Relevant clinical history and physical exam:
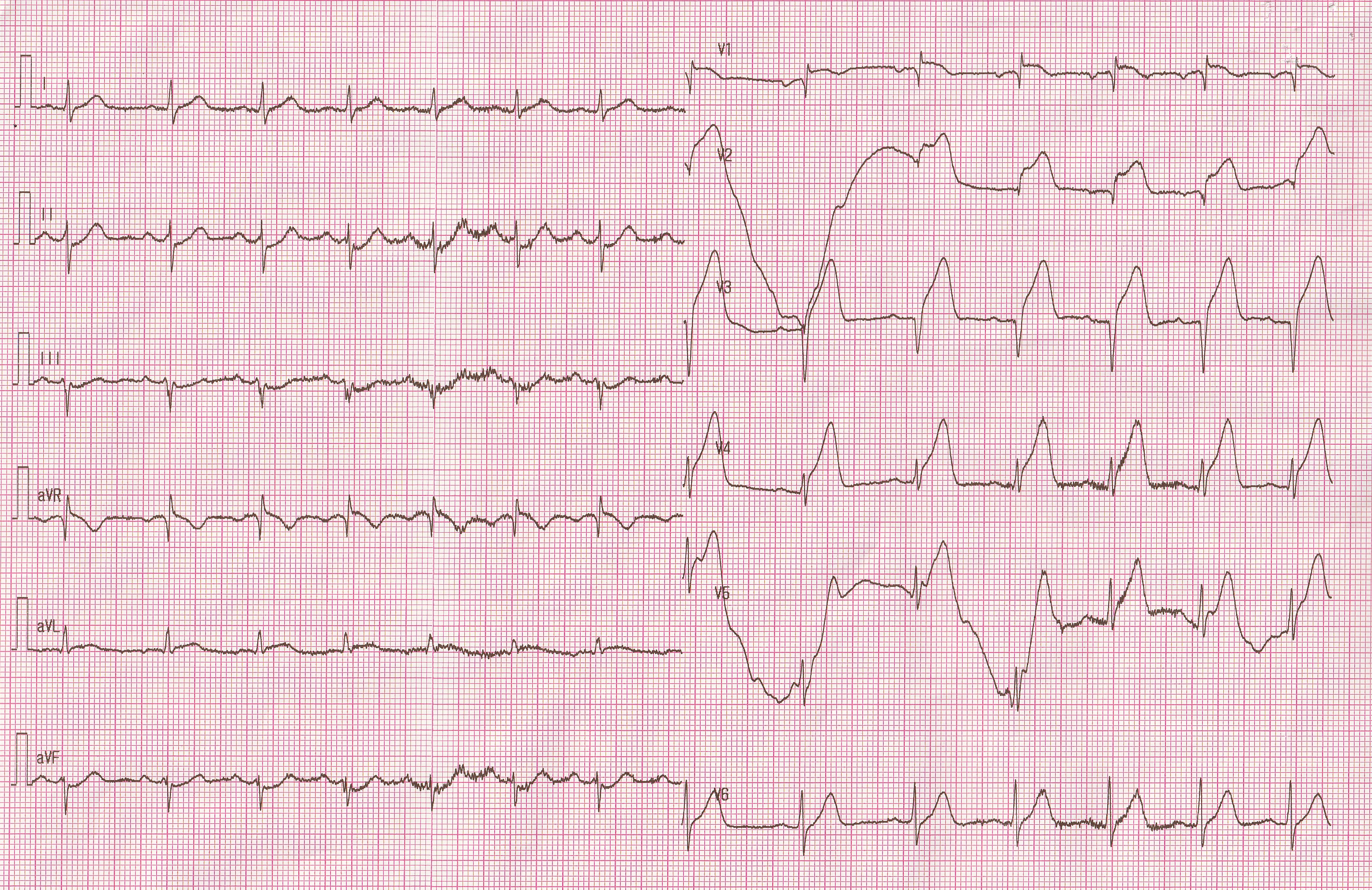
In the middle of the night, 54-year-old man came to our emergency department because he had substernal chest pressure for two hours. It come when he was sleeping. In the past two months he often felt chest pain that relief by itself. He only had diabetes mellitus. ECG showed ST elevation in V1 – V4. Fibrinolytic therapy was given due to Primary PCI is unavailable. But in the morning, chest discomfort is getting worse and ECG showed paroxysmal atrial fibrillation. Rescue PCI was planned.
 -Relevant test results prior to catheterization:
Echocardiography demonstrated reduced motion in anterior region, with EF 57%. Leucocyte was 11.700 μL. HbA1C 5.9. Qualitative Troponin I was negative. Post-fibrinolytic ECG didn't show any decrease in ST segment.
 - Relevant catheterization findings:
Coronary angiography revealed total occlusion in the proximal of LAD and collateral supply from RCA
|
|
|
[Interventional Management]
- Procedural step:
A 6Fr sheath was inserted through right femoral artery. Multiple views of LCA was performed. Target lesion was noticed in proximal of LAD. Multiple views of RCA showed presence of collateral branch from RCA to LAD. Using antegrade approach we successfully cross the CTO lesion with guide wire Fielder XT 0.014. We tried to predilate with balloon Across CTO 1.1x10 mm and continue predilate with bigger balloon, Pantera 2.0x15 mm, in several times. After compress the stenotic lesion we saw milking effect in the next part of the CTO lesion, and conclude that it is myocardial bridging. With classic technique, Enviros 2.5x29mm was successfully cross the lesion, and inflated up to 13atm, and the procedure was completed. We decided to didn't do any stenting in myocardial bridging and observed for further improvement by aggressive pharmacological therapy. - Case Summary:
In this case, the myocardial bridge has responsibility for the development of atherosclerotic plaque. Fluid mechanics disturbance in proximal part of myocardial bridge play in an important role for the development of atherosclerotic plaque which grows into CTO lesion. Low wall shear stress level in this area increase VCAM-1 expression, Reactive Oxygen Species, and proatherogenic endothelial. CTO lesion was successfully stent without any residual stenosis. Furthermore, we decided to treat Myocardial Bridge with aggressive pharmacological therapy, include CCB, antiplatelet, and statin, rather than do stenting in the myocardial bridge. |
|