Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191115_003
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Impact of Jailed Corsair Technique for the Complex Bifurcation Lesion | |
| Atsuichiro Shigenaga1 | |
| Tokyo Heart Centnr, Japan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
MT
-Relevant clinical history and physical exam:
A 92-year-old woman presented with acute chest pain for two hours. She has hypertension and dyslipidemia as coronary risk factors. Initial blood pressure at emergency room was 93/60 mmHg and heart rate was 62 bpm. Chest auscultationfindings was Killip II.
-Relevant test results prior to catheterization:
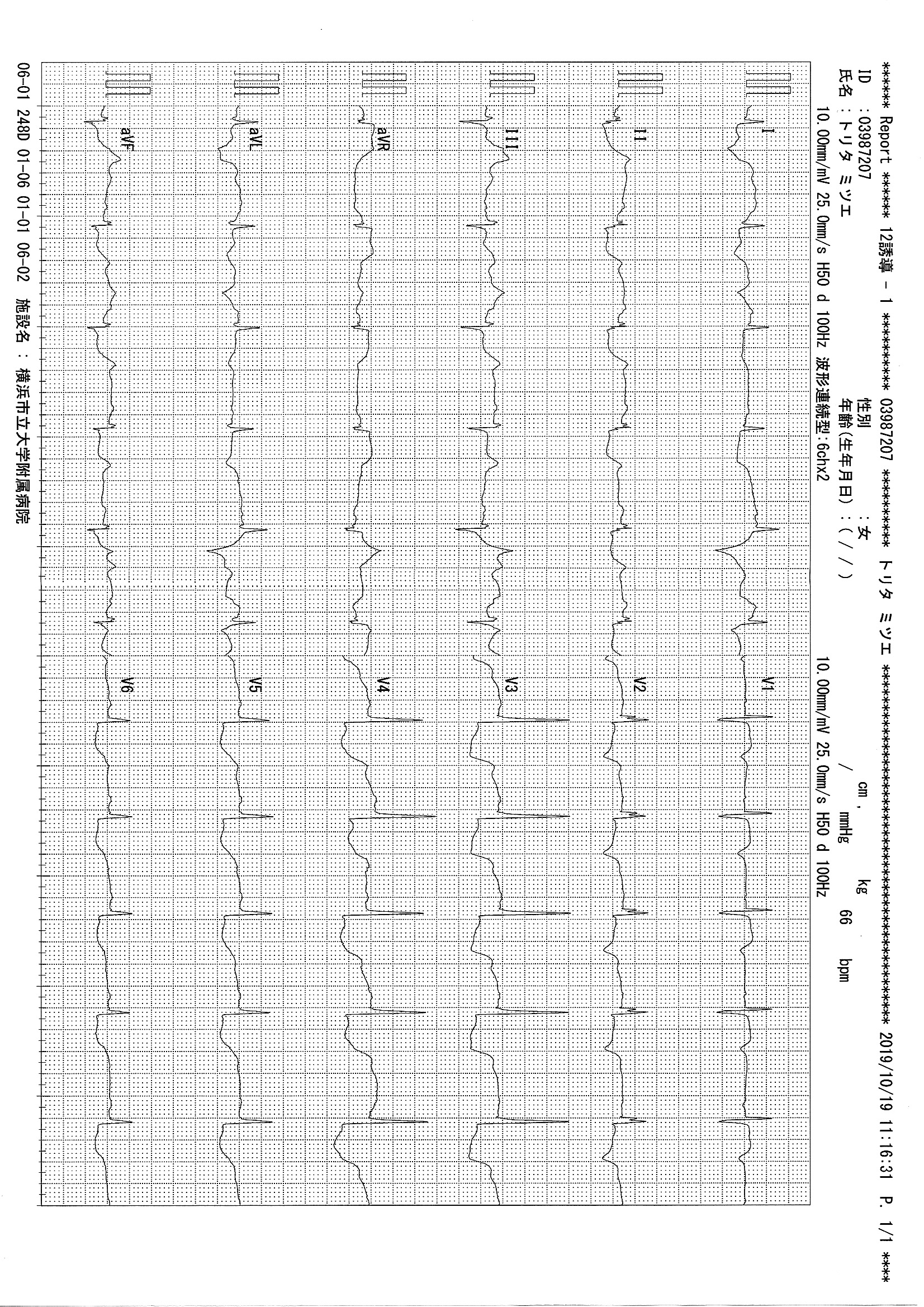
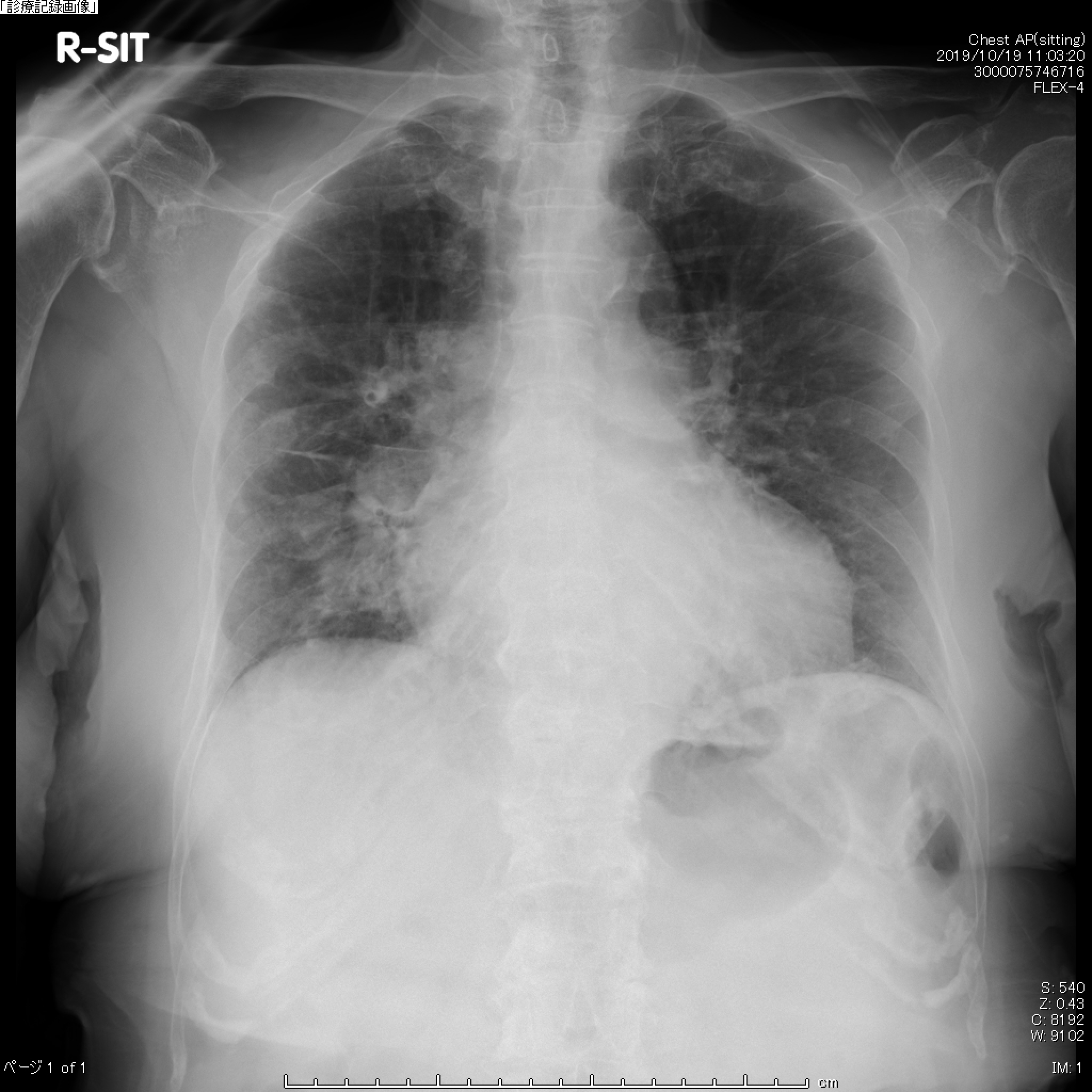
Baseline ECG showed ST segment elevation in aVR, and depressions in lead I, II, III, aVF, and V2-6. The Chest X-ray findings were congestion and cardiac dilatation (CTR=55%). The echocardiography revealed reduced left ventricular function (EF=40%) with mid anteroseptal wall motion abnormality and moderate MR. Cardiac enzymes included CK-MB were elevated (CK420 U/L and CK-MB 53 U/L). Renal function was normal. She underwent emergency coronary angiography for primary angioplasty.
  - Relevant catheterization findings:
|
|
|
[Interventional Management]
- Procedural step:
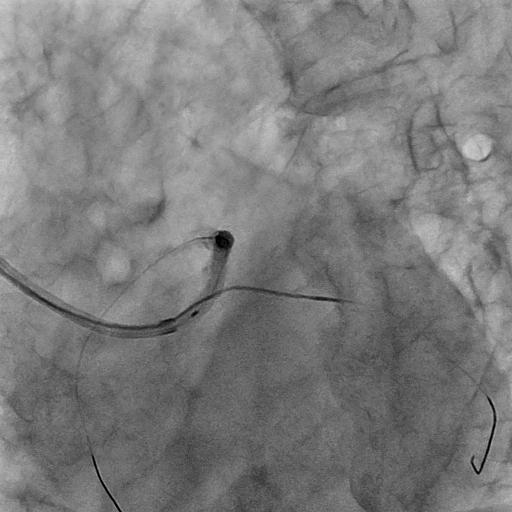
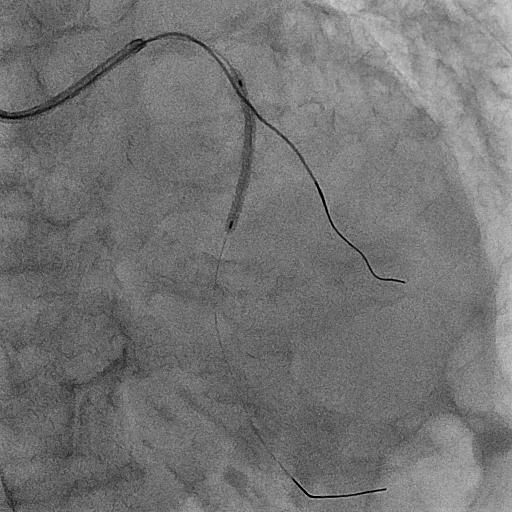
An 7Fr GlideSheath Slender was inserted through right radial artery, and an 7Fr JL 3.5 guiding catheter with side hole was engaged after IABP insertion. The 0.014” SION wire was inserted into the LAD and the 0.014” SION Blue wire into the LCX. First, we checked LM bifurcation with intravascular ultrasonography (IVUS), which showed heavy plaque. After predilatation with Scoreflex NC 2.75x15mm, TIMI 3 flow was acquired. Then, XienceSierra 3.0x33mm was deployed at LM to prox LAD with jailed Corsair technique (JCT)with purpose of the secure LCX protection and avoidance of the LCX dissectiondue to ballooning. Finally, proximal optimization technique (POT) with NC Euphora 4.0x6mm, kissing balloon inflation (KBI) by Scoreflex NC 2.75*15mm and SeQuent Please 2.5*15mm, and rePOT were done well. Final angiography revealed good result. Fractional flow reserve (FFR) value at the distal LCX was 0.55, but no jump up at the proximal site. One week later, calcified mid LAD including the narrowing diagonal branch was treated via 7Fr transradial approach. Optimal coherence tomography (OCT) catheter was not passed despite of Guidezilla support, so debulking by Orbital atherectomy system (OAS) was needed. Next, we performed predilatation with Wolverine 2.5*10mm under the wire protection of the side branch, and deployed Xience Sierra 2.5x33mm overlapped the proximal stent using JCT. The sandwiched Corsair by the stents was safely retrieved. Final angiography was good result.
  - Case Summary:
JCT could overcome concern about jailed balloon technique, which is balloon stuck, rupture, and the side branch dissection. Especially, it is useful for the emergent case with unstable hemodynamics to protect the side branch without dissection. Furthermore, this technique is safe in the situation of sandwiched stents.
|
|