Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191114_011
| STRUCTURAL HEART DISEASE - Others (STRUCTURAL HEART DISEASE) | |
| Down the Rabbit Hole | |
| Thinnakrit Sasiprapha1, Krissada Meemook2, Mann Chandavimol1 | |
| Ramathibodi Hospital, Thailand1, Ramathibodi Hospital Mahidol University, Thailand2, | |
|
[Clinical Information]
- Patient initials or identifier number:
PP
-Relevant clinical history and physical exam:
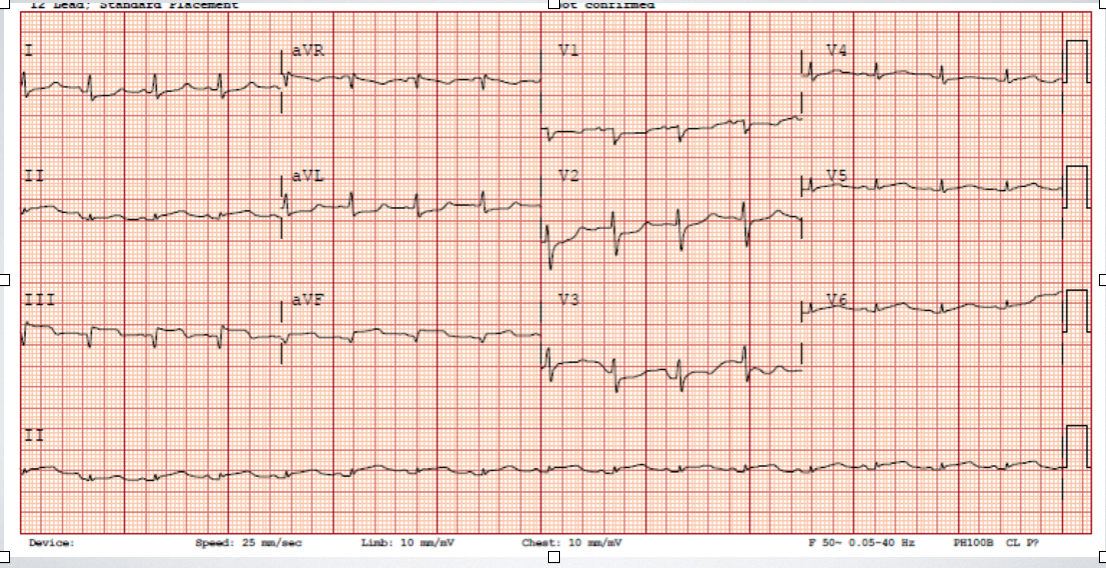
A 53-year-old female presented with chest pain for 1 day. ECG had ST-elevation on inferior leads. Emergency primary PCI was done at the proximal RCA. The next day, she deteriorated with congestive heart failure. New pansystolic murmur was detected. Ventricular septal pseudoaneurysm with ruptured was diagnosed. Device closure with PDA occluder was done with residual defect. Surgical closure was urgently performed with patch, residual defect still persisted and the patient was not improved.
 -Relevant test results prior to catheterization:
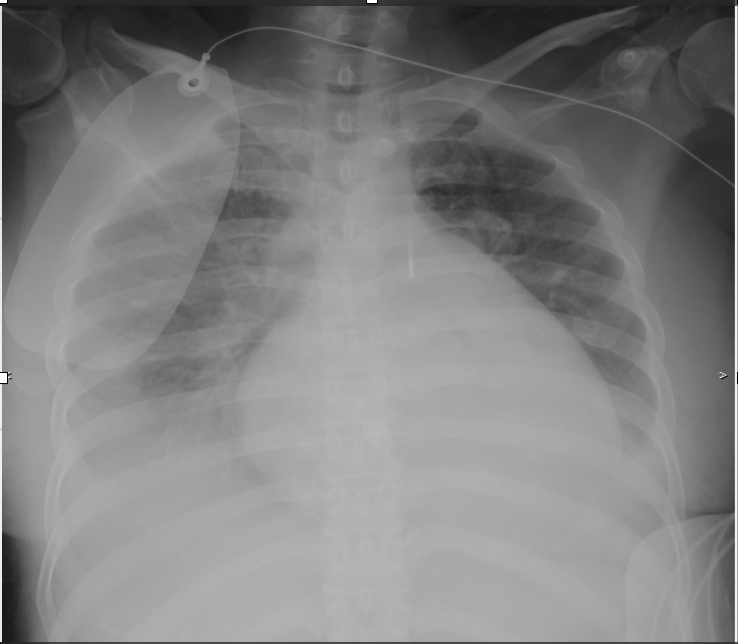
A chest X-ray showed increased pulmonary vasculature with bilateral pulmonary edema. An echocardiogram revealed ventricular septal pseudoaneurysm with ruptured (Qp:Qs 2.2:1) was found on echocardiogram.
 - Relevant catheterization findings:
The baseline left ventriculogram demonstrated abnormal contrast flow from left ventricle to right ventricular with large pseudoaneurysm. After a 26 mm cocoon PDA occluder device was deployed, there was still significant residual defect. She was then undergoing semi-urgent surgical repair using pericardial patch. Post-surgical repair, left ventricular ventriculogram, again, revealed large left to right shunt through the defect.
|
|
|
[Interventional Management]
- Procedural step:
A 6 Fr sheath was inserted into right femoral artery and 7Fr sheath was inserted to right internal jugular vein. The Terumo wire was inserted from LV to RV and then to PA. The Terumo wire was snared by Multi-snare catheter then externalized via right jugular vein for making an AV loop. 10 Fr delivery sheath was inserted antegradly from the right internal jugular vein to LV. The Terumo wire was then removed. Amplatzer muscular VD occluder16 mm prepped and loaded into deliver system using fluid-to-fluid technique. The device was deployed across the VSD under fluoroscopic and TEE guidance. Seating of the device was tested to ensure a stable position. TEE and left ventriculogram still showed significant residual left to right shunt. 0.025" Terumo wire with JR catheter were used to cross the residual VSD from LV then into PA and the wire was snared by Multi-snare to internal jugular vein. A 6.5 Fr JR 3.5 Sheathless guiding catheter was advanced over Terumo wire and could pass the residual defect retrogradly(after failure to pass antegradly) via right femoral artery. Amplatzer vascular plug II 12 mm was prepped and then deployed across the residual VSD. TEE showed small residual CDF across septum and Qp:Qs markedly decrease from 2.8:1 to 1.1 : 1. The device was checked for stabilization and then securely detached.
- Case Summary:
This case demonstrated a transcatheter technique for treatment of post-infarct ventricular septal rupture after surgical closure failure. The key steps for successful treatment were combined antegrade and retrograde approach for different devices, using 6.5 JR Sheathless instead of introducer sheath due to softer and more tapering tip and using the second device with more apical deployment.
|
|