Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191114_010
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Primary Percutaneous Coronary Intervention (PPCI) in Native Vessel Following Saphenous Vein Graft (SVG) Failure: An Important Role for Coil Embolization | |
| Robert Thomas Gerber1 | |
| Nepean Hospital, Australia1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mrs AG
-Relevant clinical history and physical exam:
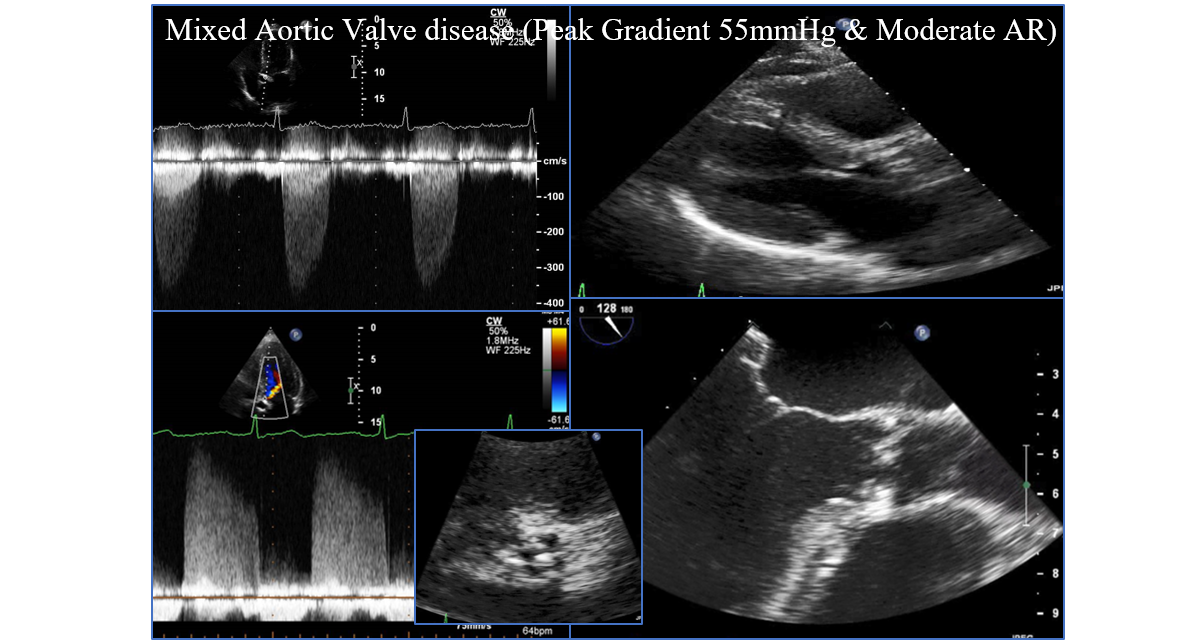
78-year-old lady with hypertension, osteoarthritis and gastroesophageal reflux disease presented to her primary care physician with increasing dyspnoea and reduced exercise capacity. She had a clear ejection systolic murmur and high pitched early diastolic component. and subsequent transthoracic and transoesophageal echocardiography demonstrated mixed aortic valve disease. She had a peak gradient of 55mmHg and moderate aortic regurgitation (Figure 1).
 -Relevant test results prior to catheterization:
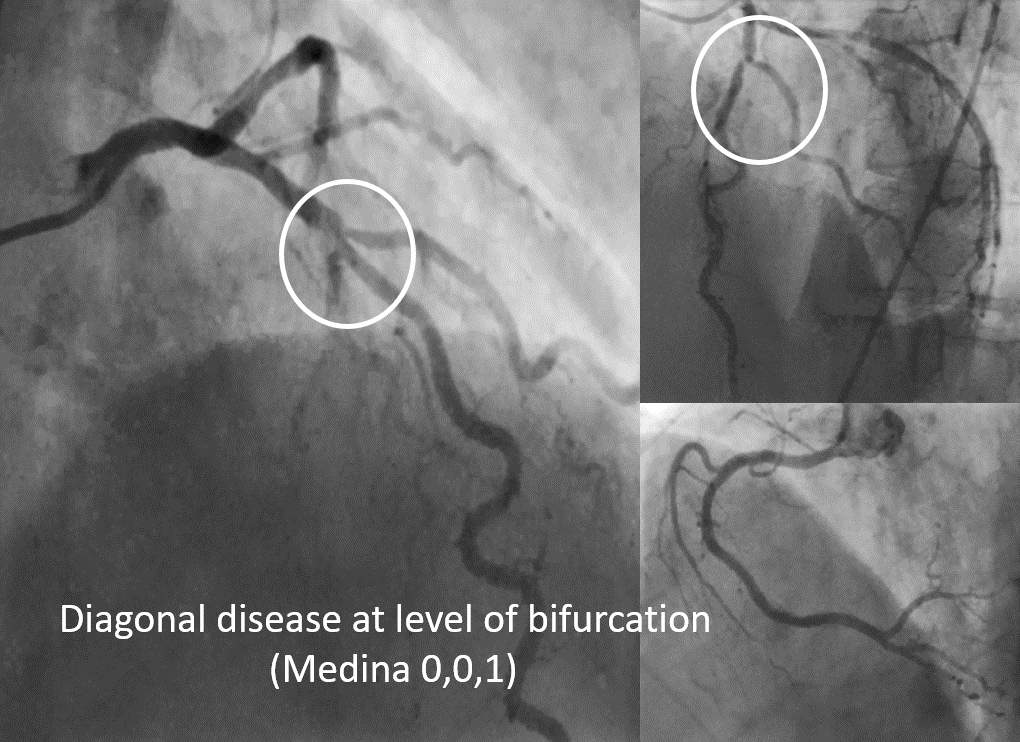
Coronary angiography demonstrated more or less normal coronary vessels apart from an ostial pinch at the level of the diagonal (Medina 0,0,1) (Figure 2). Her case was discussed at the cardiosurgical multi-disciplinary meeting and accepted for surgical repair of Aortic Valve (bioprosthetic) with single vessel saphenous vein graft (SVG) implanted on the diagonal vessel. She had intermittent complete heart block post AVR so a PPM was implanted.
 - Relevant catheterization findings:
She was free of dyspnoea but 5 months post-procedure had chest pain whilst in the Post Office. She then sustained an out of hospital cardiac arrest with bystander CPR performed and public access defibrillation. Return of spontaneous circulation was eventually achieved (ROSC) and ambulance ECG demonstrated lateral ST elevation. She was transferred for PPCI with haemodynamic instability .Angiography demonstrated occlusion of the diagonal SVG at the insertion site with retrograde filling of the SVG.
|
|
|
[Interventional Management]
- Procedural step:
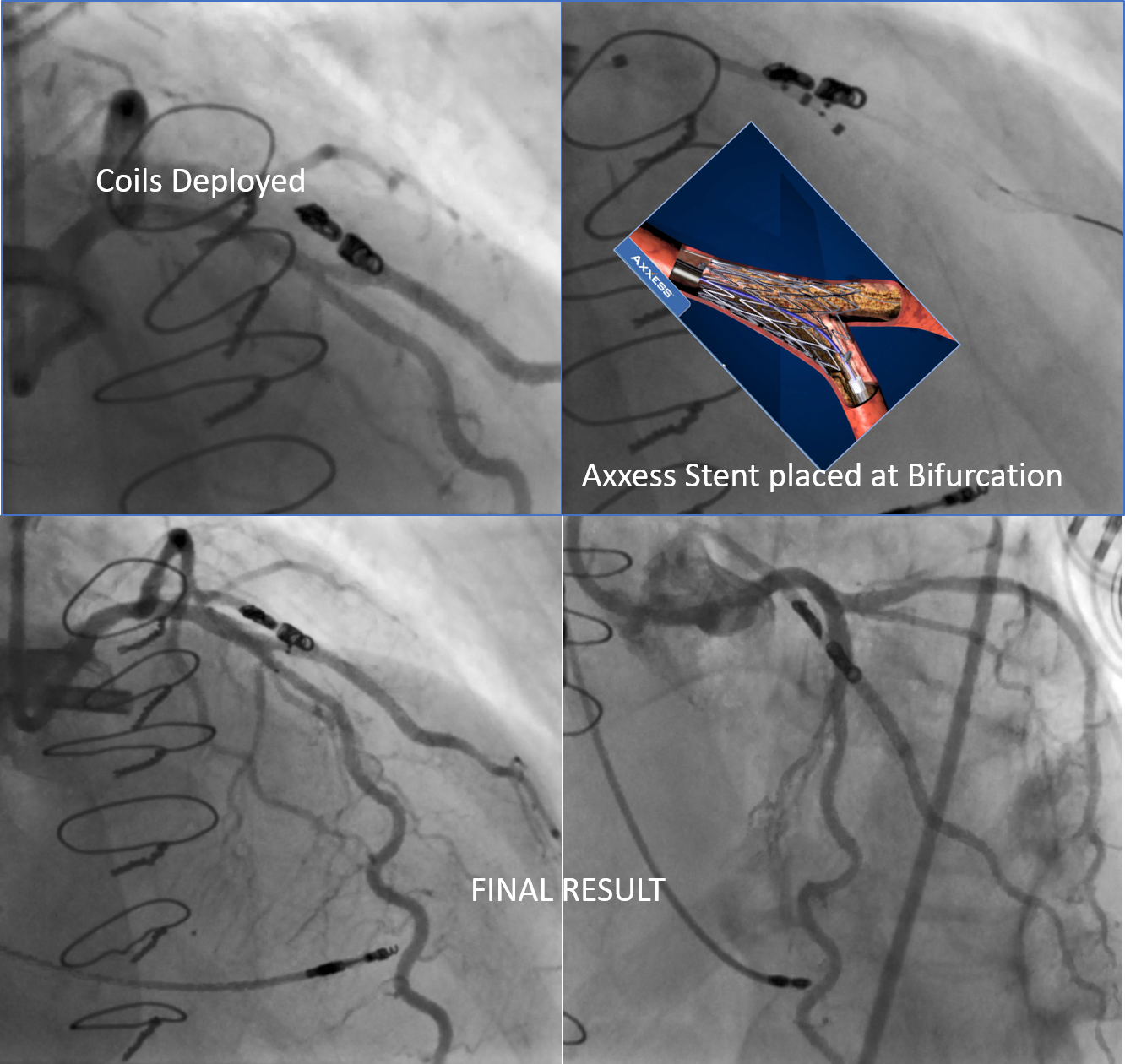
The initial strategy was to restore TIMI III flow into this diagonal. We suspected that the cause for the occlusion was due to an anastomotic stenosis at the junction between the SVG and its insertion into the diagonal. Therefore, the aim was to restore antegrade flow through the native circulation and perform bifurcation PCI into the diagonal. The native LAD and diagonal were wired with Runthrough wires(Terumo) and a thrombus aspiration catheter was placed but it actually did not traverse through the bifurcation and was held up at the ostium of the diagonal. Nevertheless, TIMI 3 flow was restored and the vessel was pre-dilated with a 2.0x20balloon and then stented with a 2.5x26 Resolute Onyx (Medtronic). Despite stenting flow was compromised into the distal vessel with persistent competitive flow observed retrogradely into the SVG. In order to facilitate native antegrade flow the SVG was occluded with the use of an AL1 guide and a Progreat microcatheter and several Cook embolization coils. The coils were implanted within the SVG with the use of a proximal occlusion balloon adjacent to the microcatheter to prevent proximal migration of the coils. This restored native flow and the native vessel intervention was completed with the use of a dedicated bifurcation stent Axxess (Biosensors) implanted in the LAD and flared into the diagonal to effectively treat the native bifurcation disease. Following this haemodynamic stability was restored and the ECG changes resolved.
 - Case Summary:
This case highlights the importance of considering coil embolization of bypass grafts to facilitate antegrade flow within native coronary arteries to ensure long-term patency after native vessel PCI. This has implications for CTO revascularisation of grafted vessels as well as PCI in patients post CABG.
|
|