Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191114_009
| CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP) | |
| The Fate of Dislodged Stent Strut in Patients with CHIP | |
| Dae-Won Kim | |
| , | |
|
[Clinical Information]
- Patient initials or identifier number:
JCS
-Relevant clinical history and physical exam:
chief complaint : mild DOE, admitted for preoperation evaluation for Rt. inguinal herniaPast history : DM/PAF/HTN (-/-/-)FHx. : n/sSHx : n/slab. : BUN/Cr 9.7/1.15, WBC 6000, LDL 163, Hb 13.8, TC 235, proBNP 1246
-Relevant test results prior to catheterization:
ECG ; RSR, LVHCXR : CP blunting Lt.TTE ; EF=27% with ischemic insult in multiple territory
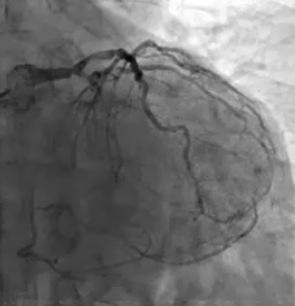 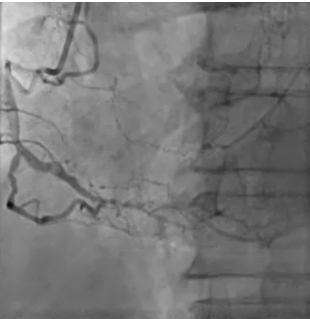 - Relevant catheterization findings:
LM bifurcation, LMos significant lesion, LM to pLAD severe calcification, RCA &LCX CTO, R/O dRCA thrombosis-> CHIP
|
|
|
[Interventional Management]
- Procedural step:
1. LM bifurcation with LMos, p to mLCX & p to mLAD1) GC : 7Fr EBU 3.5-SH2) Wire : RUnthrough wiring into dLAD3) IVUS : diffuse severely calcified (270~360 arc) fibro-fatty atheromaat p to mLADWe are planned to perform LM PCI first following cautiously trying LCX CTO PCI with the possibility of distal embolization during LCX CTO interventiondue to eccentric fibro-calcified plaque in LMos
=> Stent at LM : Orsiro 4.0-15mm uptpo 20 atm at LMos to LM shaft * LCX CTO intervention * * LAD rotablation & preballooning at LAD& LCX with LM bifurcation *7) Wire ; Runthrough with Finecross into dLADWire exchange with Rota wire 8) Rotablation : 1.75MM burr upto 173000 RPM at mLAD 3 times9) Post IVUS : partly cracked calcified plaque 10) Wire exchange with Runthrough * LM bifurcation 2 stent mini-crushing technique *11) Fielder XT wire into LCX and ballooning 12) Balloon : Ikazuchi 3.0-10mm upto 14 atm at LCXos to mLCXIkazuchi ballooning 3.0-10mm upto 14 atm at LM to pLAD13) Stent : Orsiro 3.0-22mm upto 14 atm at p to mLCXOrsiro 3.0-26mm upto 14 atm at mLAD 17) Final kissing ballooning, POT with double ballooning :Emerge NC 3.5-12mm at LM to pLCX & Emerge NC 3.5-12mm at LMto pLAD upto 6 atm Emerge NC 3.5-12mm upto 18 atm at LM for POTEmerge NC 3.5-12mm & Emerge NC 3.5-12mm (double ballooing) 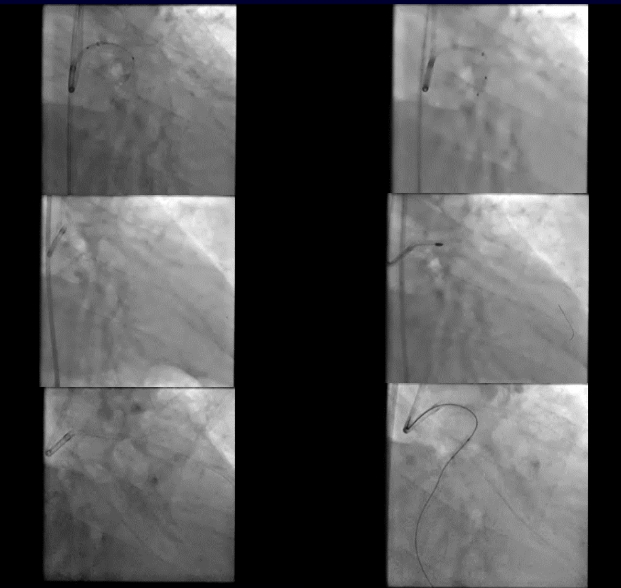 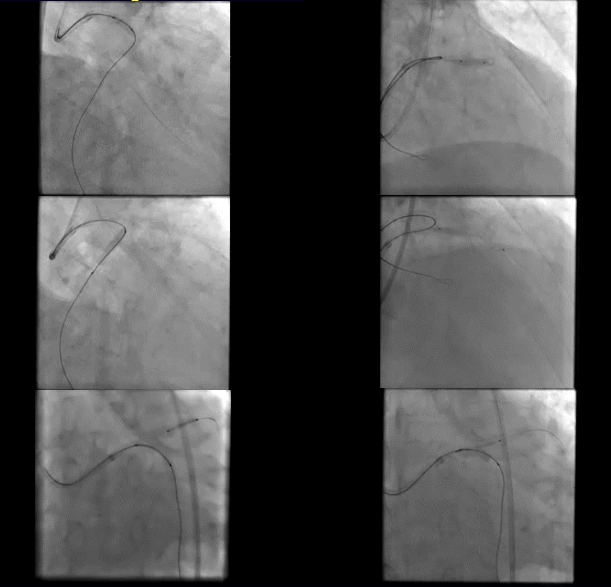 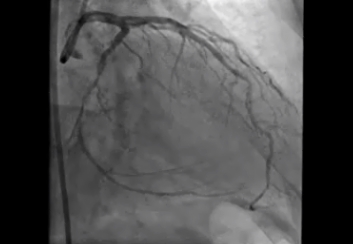 - Case Summary:
This case CHIP which include LM bifurcation, LMos significant lesion, LM to pLAD severe calcification, RCA& LCX CTO, dRCA thrombosis. Folling refusing to do CABG, I decided to proceed PCI. After successful RCA PCI at index, I performed staged PCI for LCX CTO, LM bifurcation, LMos significant lesion and LM to pLAD severe calcification with LM bifurcation with rotablation and CTO PCI. However, Dislodged stent occurred during PCI was found in the superior segmental artery of Lt. renal artery in the next day. I checked with abdomen CT, fluoroscopy in Cath Lab and found no flow limitation, well arterial flow into renal space stuck with stent strut. Afterwards I’m onging follow-up without removal.
|
|