Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191114_006
| ENDOVASCULAR - Peripheral Vascular Disease and Intervention | |
| A Novel Technique Using a Guide Extension Catheter for Acute Limb Ischemia in the Non-Stenting Zone | |
| Yamane Haruya1 | |
| Otemae Hospital, Japan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
C.K.
-Relevant clinical history and physical exam:
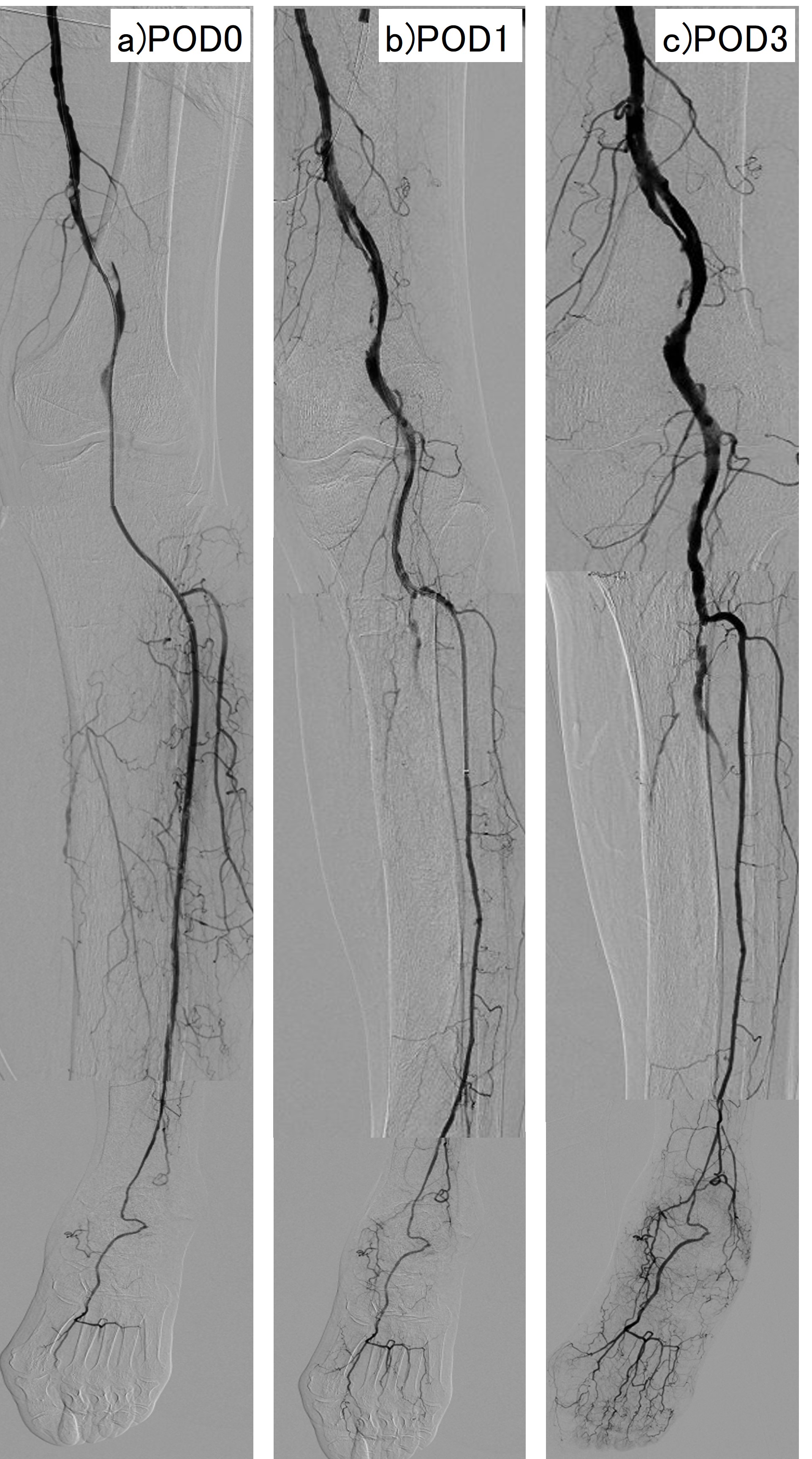
An 83-year-old female was transferred to our hospital for acute rest pain and coldness in her left lower leg, which was occurred 2 days before. On admission, her left lower leg showed ischemic changes; paleness, pulselessness and coldness. She had no medical history of atrial fibrillation or embolism.
 -Relevant test results prior to catheterization:
The Doppler couldn’t detect any pulse of the left lower limb arteries. The ankle brachial index of her left leg was unmeasurable, and the lower extremity ultrasonography revealed an obstruction of the left popliteal artery. The laboratory examination findings were as follows; creatine phosphokinase 2517IU/L, creatinine 1.2mg/dL, and D-dimer 13.0μg/mL.
- Relevant catheterization findings:
The angiography revealed a total occlusion in the left popliteal artery. The IVUS image showed a lot of thrombus in the lesion, so we thought that EVT procedure including catheter aspiration or balloon dilation were not effective. A thrombectomy using a Fogarty catheter was also not applicable because a vessel dissection or distal embolization could easily occur in the narrow arteries.
|
|
|
[Interventional Management]
- Procedural step:
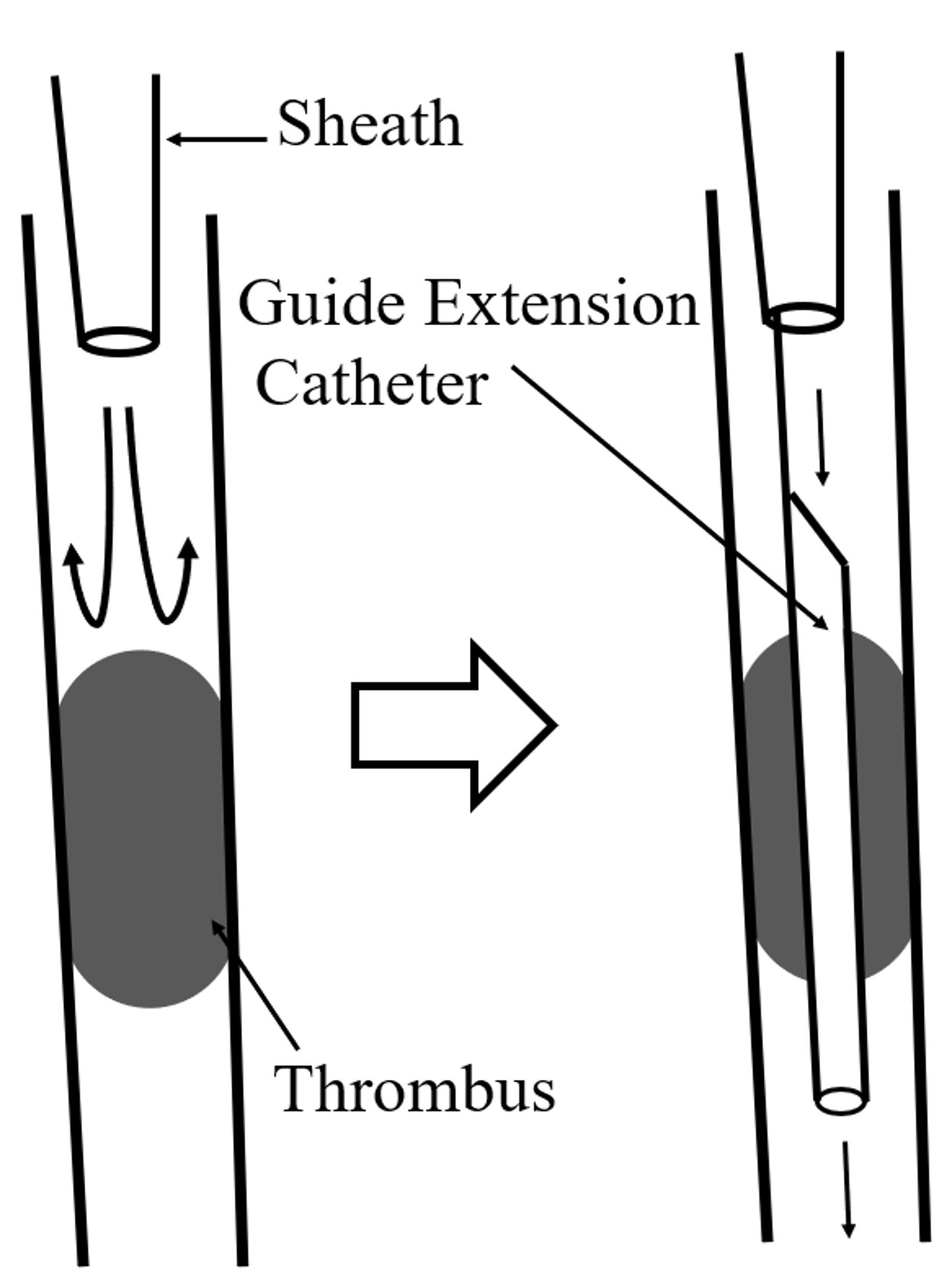
we performed our novel technique, which is temporary deployment of the guide extension catheter to the occluded lesion. First, we evaluated the lesion length or vessel diameter by IVUS or angiography. Then, we delivered the guide extension catheter to cover the occluded lesion fully with the part of the silicon tube and confirmed the blood flow to the below-the ankle arteries. Finally, a thrombolytic drug was administrated intra-arterially. On postoperative day 2, the blood flow was maintained without any flow limitation after removing the guide extension catheter. She was discharged without any additional interventions or complications.
  - Case Summary:
We developed a novel technique to treat ALI in the non-stenting zone using a guide extension catheter and administrating a thrombolytic drug. This technique prevents limb ischemia and promotes the reduction of thrombus effectively. It can be considered for treatment of ALI in the non-stenting zone.
|
|