Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191114_004
| CORONARY - Chronic Total Occlusion | |
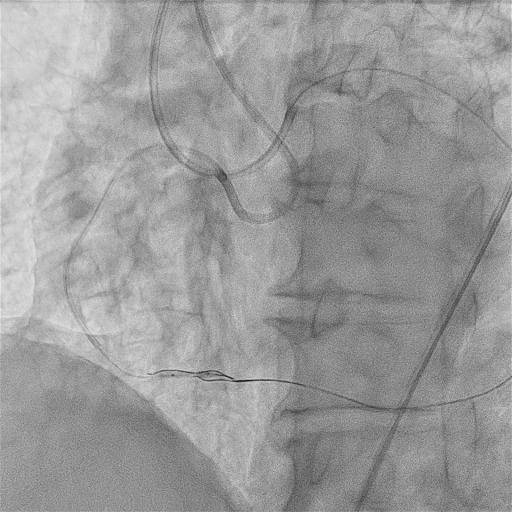
| Successful PCI for RCA Chronic Total Occlusion (CTO) with Knuckle Wire and Reverse CART Technique | |
| Yukihiro Yamaguchi1, Toshiya Muramatsu2, Reiko Tsukahara3, Masatsugu Nakano3, Hideyuki Takimura3, Mami Kawano3, Emi Tajima3, Yosuke Komatsu3 | |
| International University of Health and Welfare, Japan1, Tokyo Heart Center, Japan2, Tokyo General Hospital, Japan3, | |
|
[Clinical Information]
- Patient initials or identifier number:
HK
-Relevant clinical history and physical exam:
A case was 70 years old male, admitted to the previous hospital due to anterior STEMI in January 2019. The electrocardiogram (ECG) and emergency coronary angiography (CAG) showed the culprit lesion was seg.7 and EES was implanted. CTO was also revealed at the middle RCA and staged PCI was performed in June 2019. It was approached from only antegrade and failed. After discharge, he was referred to our hospital in July 2019.
-Relevant test results prior to catheterization:
ECG showed normal sinus rhythm, there were abnormal Q in V1-4 and ST depression in V4-6. Echocardiogram showed left ventricular ejection fraction was 26% (modified Simpson’s) and the wall motion was anterior akinesis, posterior hypokinesis. LV end diastolic/systolic diameter were 62/53 mm, secondary mild MR and mild TR were observed. Laboratory test showed Hb14.8 (g/dL), Cr 1.2 (mg/dL), eGFR 42 (mL/min/1.73m2), BNP 240 (pg/dL), HbA1c 8.4 (%), LDL cholesterol 83 (mg/dL).
- Relevant catheterization findings:
We performed prior CAG, it showed there were diffuse tandem lesions on seg.1, 2 and CTO in the middle RCA. The entry point was tapered, the calcification was absence. The lesion was not so tortuous and with no bifurcation. The length of the CTO was about 30mm (J-CTO score 2). LCA was intact, including the stent site. There were some collaterals via 1st and 3rd septal and diagonal branch, they were not jailed by the stent. We planned to a staged PCI to the RCA CTO lesion.
|
|
|
[Interventional Management]
- Procedural step:
It was approached by Bi radial approach with both 6Fr Glidesheath. We used 7Fr AL1.0 SH for antegrade and 7Fr EBU3.5 SH for retrograde. At first, we attempted to cross the lesion from antegrade with XT-R and Corsair pro, but the wire went into false lumen. We stepped up the wire, GAIA 1, GAIA 2, GAIA 3, shaped the tip of the wires slightly curved to be back to the true lumen, but we couldn’t get the CTO exit. Then, we switched to retrograde approach. We chose 3rd septal channel at first. The channel was fairly straight, but narrow. We tried wire tracking with SION black, SUOH03, but they didn’t pass through. Next, we tried from the 1st septal channel. It was straight, not too narrow. We approached with SUOH03, but it went to subintimal space in distal RCA and we couldn’t reach the re-entry site of CTO. At last, we chose apex channel connected to RCA via D1 fairly. SION black and Caravel passed through the channel and reached to distal RCA relatively easily, however, we found the tip of the wire was in false lumen. So, we used the knuckle wire technique. Then we changed the wire to Ultimatebros3 and it advanced to the rendezvous point. After the reverse CART technique, Caravel from retrograde advanced to the entry site of CTO and externalization was successful. Intravascular ultrasound (IVUS) showed the wire was almost in true lumen, a part of the junction site was false but the length was within the permissible range. Finally, we implanted 4 EESs for seg.1-3 and finished.
 - Case Summary:
We constantly aware of the risk of complications, such as perforation of collateral channel, the occlusion site. In this case, two wires from antegrade and retrograde were both in subintimal space. In that situation, the knuckle wire technique was quite effective. Straight wire sometimes penetrates a vessel, but knuckled wire advances into the subintimal space without going outside of the vessel. Also, we achieved externalization with the reverse CART technique, the antegrade balloon should be as small as possible to avoid bigger dissection. We should always take minimizing the risk of complications into our account and have to expertise a lot of techniques to bail out the situations.
|
|