Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191113_014
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Percutaneous Coronary Revascularization in an Adult with an Anomalous Origin of Left Main Coronary Artery During Acute Coronary Syndrome | |
| Chamidi Siriwardane1, Gamini Galappatthy2, Anidu Keethi Pathirana Anidu Keethi Pathirana3, Naigalage Upananda Ajith Dissanayake4, Aruna Wijesinghe2, Indika Marasinghe2 | |
| National Hospital Sri Lanka, Sri Lanka1, National Hospital of Sri Lanka, Sri Lanka2, Colombo South Teaching Hospital, Sri Lanka3, The National Hospital of Sri Lanka, Sri Lanka4, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mrs W.H.J
-Relevant clinical history and physical exam:
She is a 52-year-old female with a background history of Hypertension and Dyslipidemia presented to a local hospital with acute onset ischemic chest pain for 5 hours duration. On admission she was in pain. Her BMI was 23 Kg /m2. Her pulse rate was 84 bpm. Blood pressure was 120/80 mmHg. lung bases were free of crepitation.
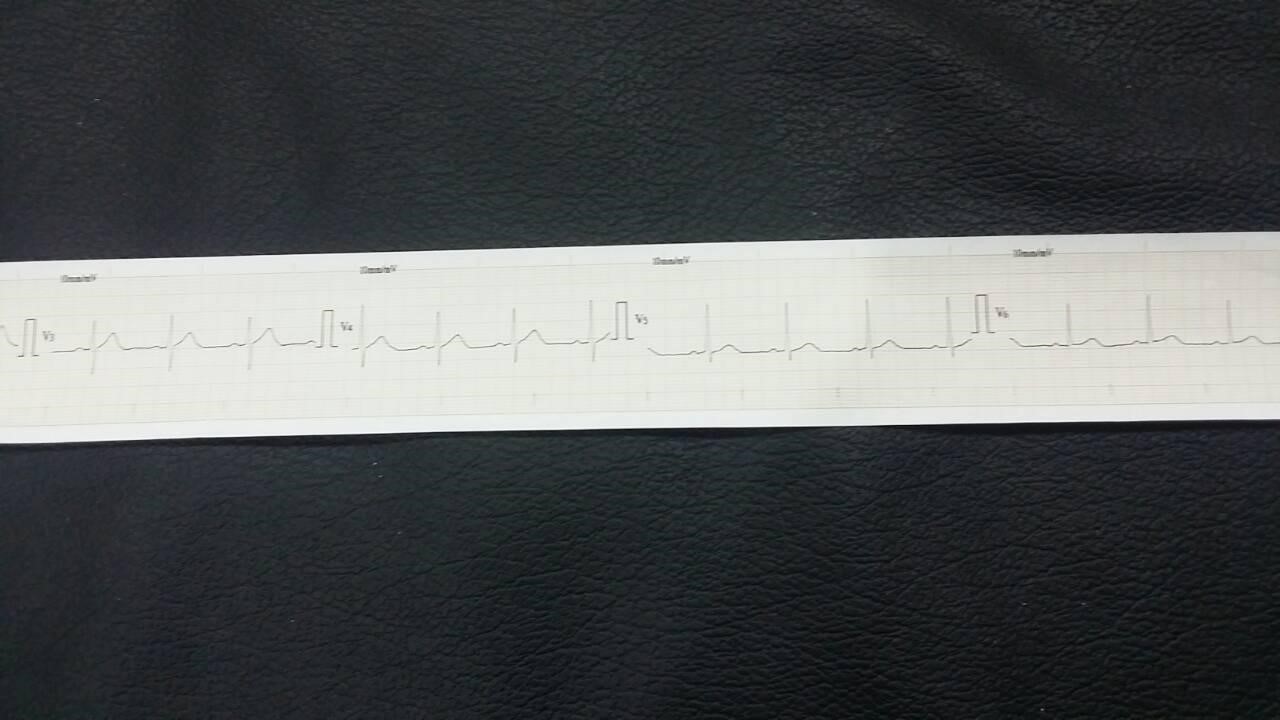
-Relevant test results prior to catheterization:
Her ECG showed ST segment elevation in inferior leads (II, III, AVF). Considering the long distance to the PCI able Centre it was decided to treat with thrombolytics. She was given tenecteplase 35 mg intravenously. Repeated ECG showed 50%resolution of ST segment in inferior leads. She was then transferred to a tertiary care Centre for coronary angiogram. Her 2D echo showed inferior wall hypokinesia. EF 50%. Normal hemoglobin and normal creatinine levels.
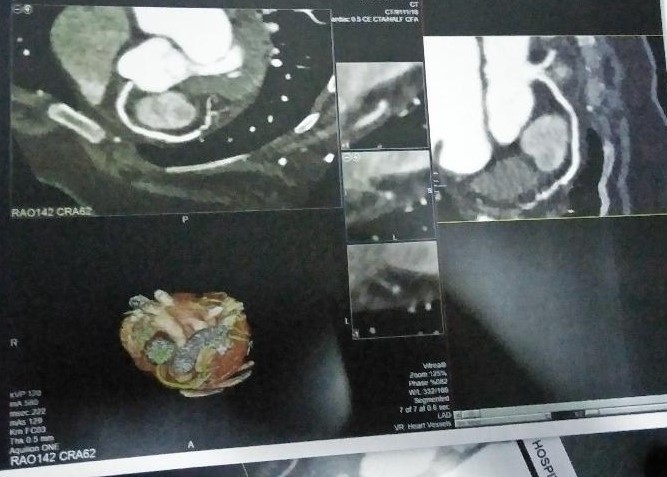
   - Relevant catheterization findings:
Her left main coronary artery was originating from right coronary cusp. LMCA long and showed mild disease. LAD showed ostial moderate stenosis .Her LCX showed ostial 90% stenosis and mid vessel 90% stenosis. RCA proximal 60%, mid vessel 90% stenosis. Since she was pain free and all vessels show TIMI 3 flow it was decided to perform a CT coronary angiogram to delineate the anomalous LMCA origin, course and relation which later discovered an pre-pulmonic course over RVOT.
 |
|
|
[Interventional Management]
- Procedural step:
Since patient denied CABG and given the fact that LMCA showed a benign course over RVOT it was decided to proceed with percutaneous revascularization. Right radial access obtained. LMCA was cannulated with JR 6 F guide catheter. LMCA TO LCX wired with a Runthrough (Terumo, Japan) 0.014'' guide wire. LCX lesion predilated with 2x 20 mm PTCA balloon. Mid LCX stented with a XIENCE PRIME 2.5x 23 mm (Abbott, US) drug eluting stent. (FD 2.7 mm). LMCA to LCX stented with another XIENCE PRIME 2.75x 23 mm (Abbott, US) drug eluting stent. (FD 3.04 mm ) overlapping with the distal stent. Overlapped segment post dilated with the proximal stent balloon. Post procedure CA show TIMI 3 flow in LMCA and its branches. RCA was cannulated with same JR 6 F guide catheter and wired with the same Runthrough (Terumo, Japan) 0.014'' guide wire. RCA lesion predilated with 2x15 mm PTCA balloon. Mid RCA stented with a XIENCE PRIME 2.75x 38 mm (Abbott, US) drug eluting stent. (FD 3.04 mm ). Proximal RCA stented with another XIENCE PRIME 3x 23 mm (Abbott, US) drug eluting stent. (FD 3.5 mm ) overlapping with the distal stent. Post procedure CA show TIMI 3 flow in RCA and its branches.
- Case Summary:
Left main coronary artery arising from the right sinus of Valsalva is the rarest coronary anomaly with the prevalence of 0.017% in angiographic series. Cardiac imaging reliably determines the proximal course and aid in risk stratification. PCI of anomalous coronaries is difficult, technically challenging and requires significant experience for successful intervention. Percutaneous revascularization is a reasonably safe and feasible option to treat diseased anomalous LMCA with a benign course particularly during acute coronary syndrome. |
|