Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191113_011
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Percutaneous Coronary Intervention to Severe Triple Vessel Disease with Total Left Main Occlusion Under Intra-Aortic Balloon Pump Support in Patient with Recent Anterior Myocardial Infarction | |
| Ho Ling Tsoi1, King Fun Tang2, Kwok Hing Yiu1 | |
| North District Hospital, Hong Kong, China1, Hong Kong Baptist Hospital, Hong Kong, China2, | |
|
[Clinical Information]
- Patient initials or identifier number:
CKS
-Relevant clinical history and physical exam:
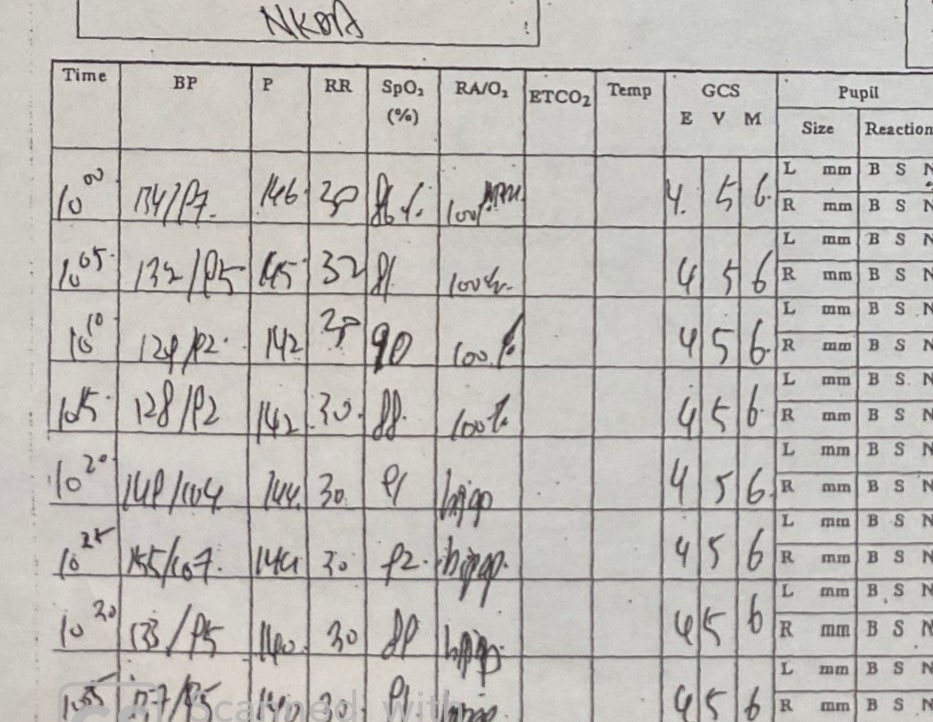
56/ M. Mr. CKS had history of HT, DM, IBD and hepatitis B. He experienced central chest pain for 10 days, which was non-exertional and was associated with dyspnea. On arrival to emergency department, his GCS was 15 / 15; BP 132 / 93mmHg; P 69 bpm; RR 26 / min; SpO2 86 % on 10 L / min O2. General physical examination showed cold peripheries and raised JVP. Chest auscultation noted bilateral basal crepitations, no audible heart murmur was heard. No lower limb edema was noted.
   -Relevant test results prior to catheterization:
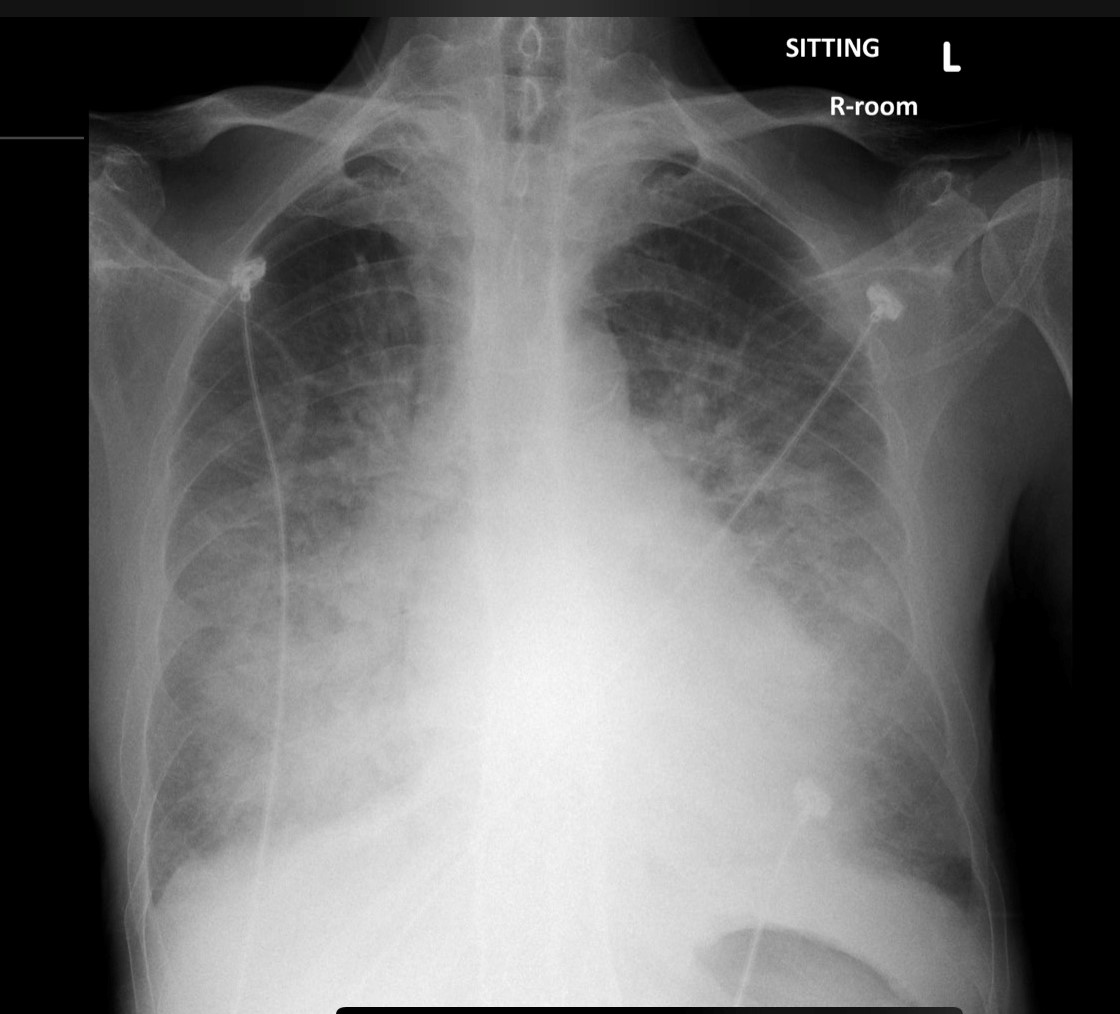
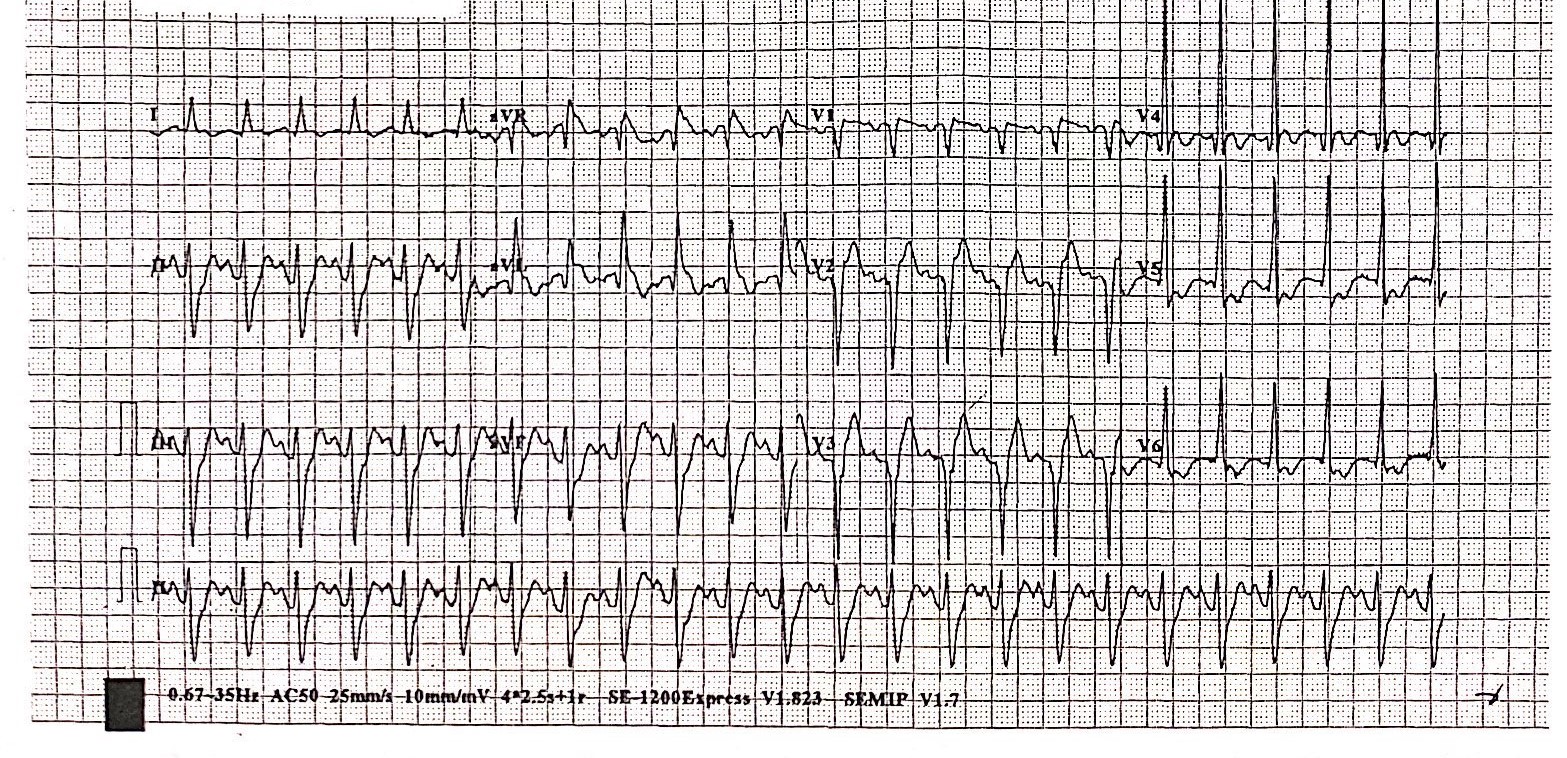
Blood capillary glucose 15 mmol / L and blood gas analysis showed type II respiratory failure. CXR: congested lung fields. ECG: sinus tachycardia 140 bpm, Q wave over anteroseptal leads with ST elevation. Bedside echo: Severe hypokinetic anterior and anteroseptal wall with LVEF 35%, mild MR and engorged IVC. Blood result revealed raised Troponin T level 871 ng / L; SCr 86 umol / L; ALT 111 U /L; Hb 14 g / dL; WBC 13 x10^9 / L. Clinical diagnosis was recent anterior myocardial infarction.
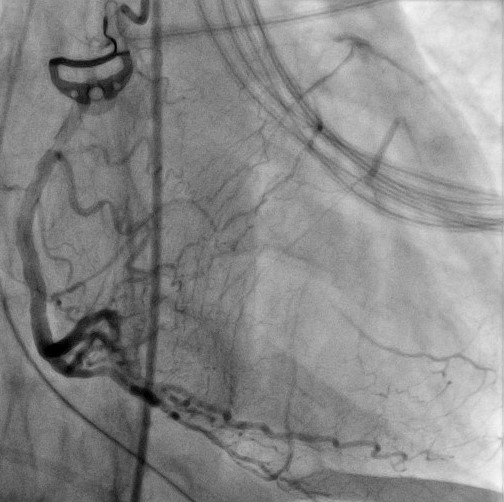
- Relevant catheterization findings:
After initial stabilization in ICU, urgent coronary angiogram was done.
  |
|
|
[Interventional Management]
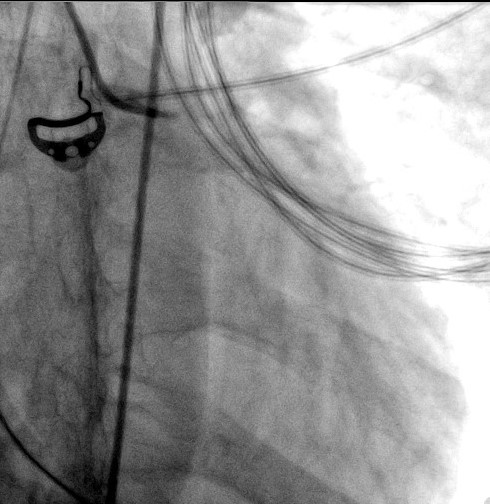
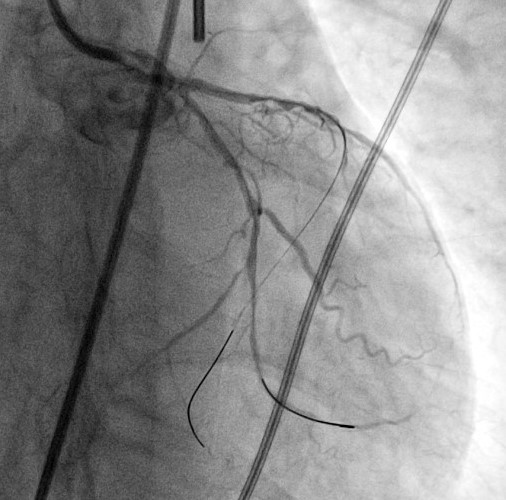
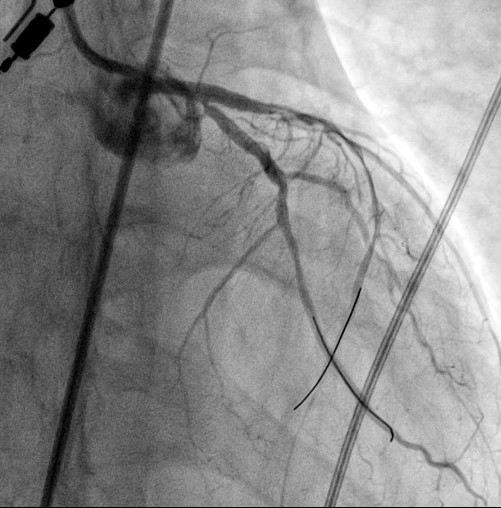
- Procedural step:
PCI was performed with femoral approach under IABP support. 6F JL4 guide was used.
  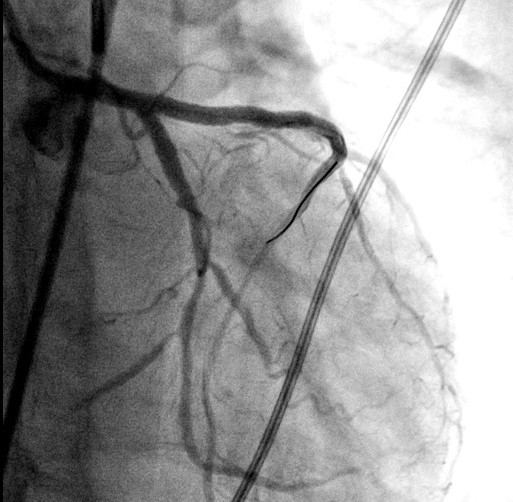 - Case Summary:
Patient eventually weaned off IABP support post PCI and heart failure medication was titrated. Cardiac rehabilitation was given post procedure and discharged home 10 days after PCI. Repeated Echo 3 months later showed improved LVEF 53% without regional wall motion abnormality.
|
|