Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191113_007
| STRUCTURAL HEART DISEASE - Valvular Intervention: Aortic | |
| TAVI in Ebstein’s Anomaly Patient and Bicuspid Aortic Valve | |
| Luca Testa1, Matteo Casenghi1 | |
| IRCCS San Donato Hospital, Italy1, | |
|
[Clinical Information]
- Patient initials or identifier number:
C.A.
-Relevant clinical history and physical exam:
A 56-year-old male, smoker, with a history of hypertension and dyslipidemia was admitted to our hospital in 2013 for acute heart failure. During hospitalization, a diagnosis of Ebstein’s Anomaly with severe tricuspid regurgitation and bicuspid aortic valve with moderate aortic stenosis was made. In 2015 after a second episode of acute heart failure a surgical correction was indicated but the patient refused. In 2017, due to a mixed cardiogenic and septic shock he was referred again to our center
-Relevant test results prior to catheterization:
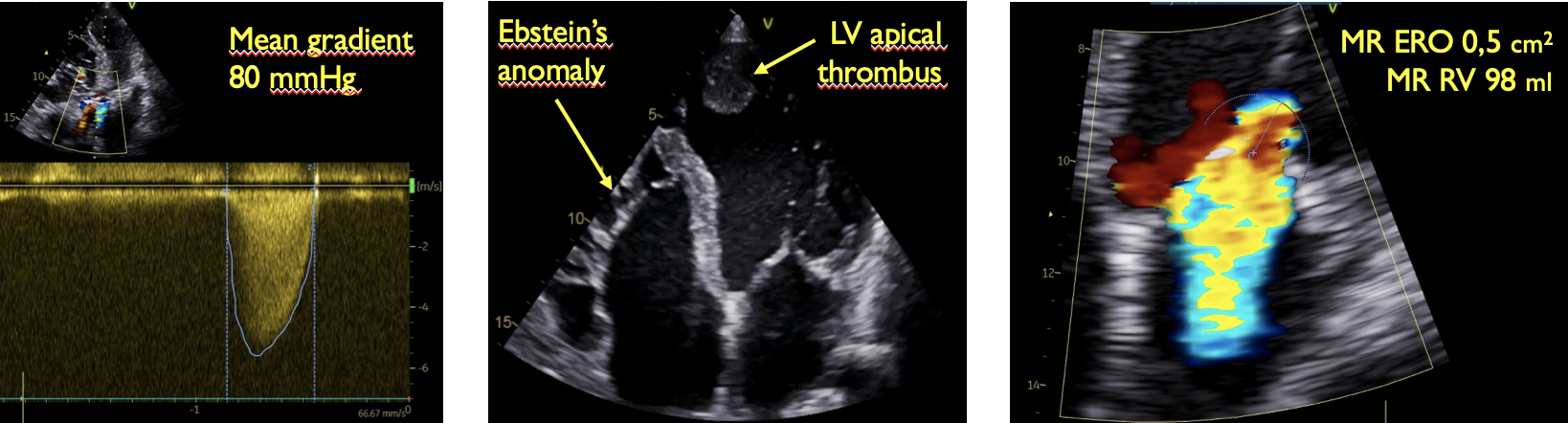
The echocardiogram showed a severely reduced LV ejection fraction (EF 20%) with severe aortic stenosis (mean gradient 80 mmHg) and severe tricuspid regurgitation (Fig.1)
  - Relevant catheterization findings:
|
|
|
[Interventional Management]
- Procedural step:
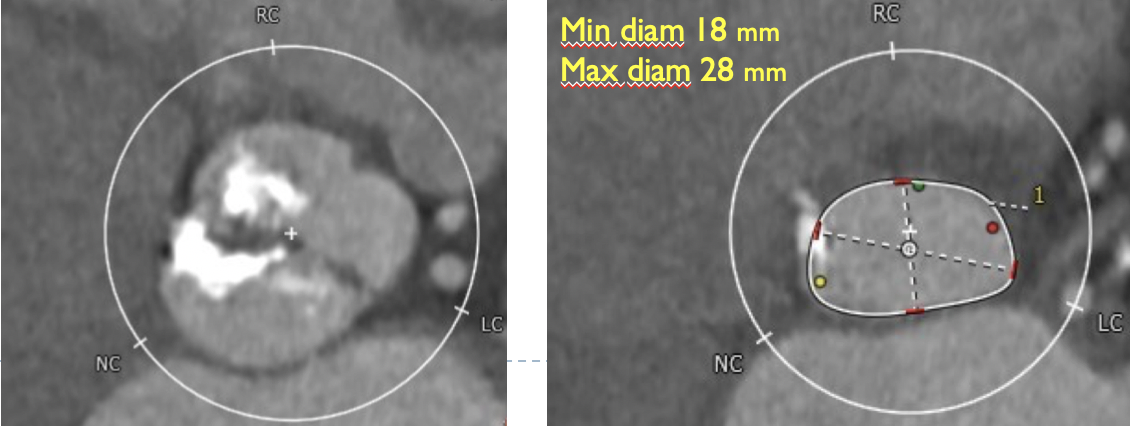
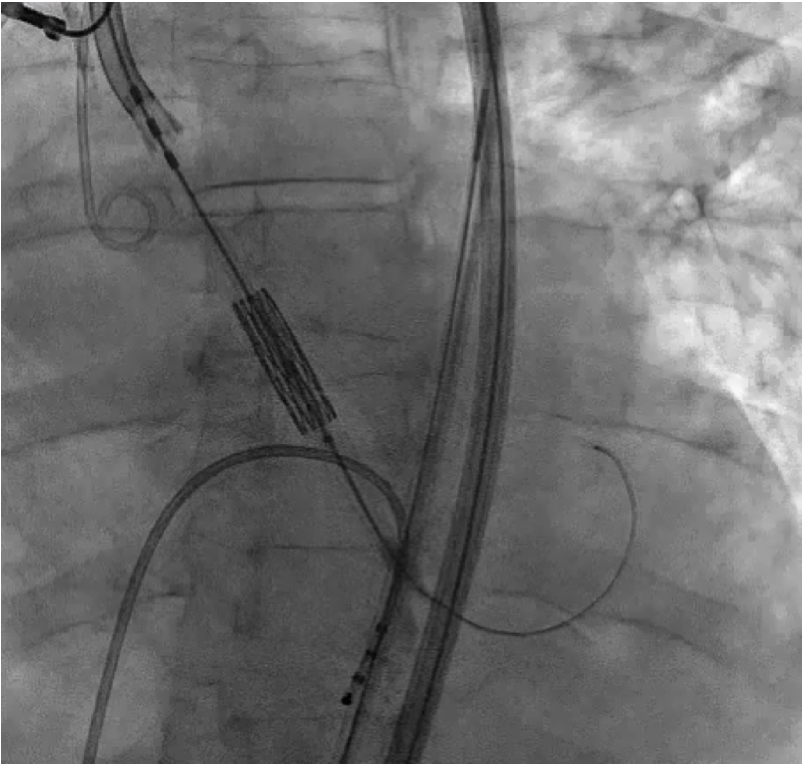
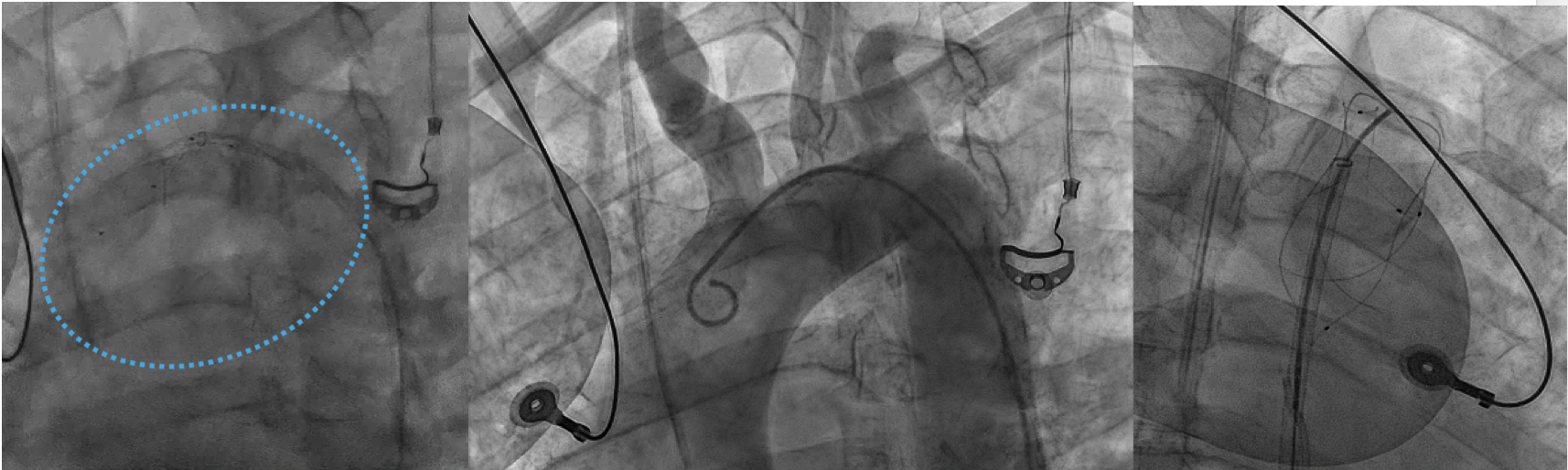
BAV, characterized by asymmetry of valve opening, extensive calcification and difficult angiographic implantation view, together with the LV apical thrombus represents a very challenging scenario for TAVR implantation. We hence planned to release a Triguard embolic protection device (Figure 1), which is the only CE marked device providing full protection of all 4 brain vessels, and to use a hand pre-formed 1 cm super-stiff wire (Figure 2) and rapid pacing to minimize thrombus mobilisation. After pre-dilatation with 21 mm a Sapien 23 mm valve overexpanded with 2 ml over-filled balloon to safely accommodate the elliptic 24 mm BAV annulus was implanted with excellent results. Three months follow-up showed good performance of bioprosthetic valve with mean gradient of 9 mmHg.
  - Case Summary:
To our knowledge is the first case of TAVI in Ebstein’s Anomaly and TAVI was a life- saving procedure in this patient. LV apical thrombus is not an absolute contraindication Embolic protection devices could be particularly useful when treating patients with LV thrombus.
|
|