Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191113_001
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Tough Call in Cath Lab | |
| Debasis Mitra1 | |
| NH-RTIICS, India1, | |
|
[Clinical Information]
- Patient initials or identifier number:
YA
-Relevant clinical history and physical exam:
51-year-old male Hypertensive, non-diabetic Complain of recurrent chest pain, jaw pain with sweating after food, sometimes angina early morning Smoker PTCA to LAD & LCX, 2nd generation DES on June 2019 ECG: Normal, V5, V6 LVEF: 65% -Relevant test results prior to catheterization:
- Relevant catheterization findings:
|
|
|
[Interventional Management]
- Procedural step:
Femoral approach JL 3.5 (6F) guide catheter SION blue PTCA Wire for LAD & for sinus for precise positioning of ostial LM stent Semi-complaint balloon for pre-dilatation 2.5*12 MM followed by 3.5*12 MM at 16 ATM Pre PCI IVUS pull back from LAD to LM - Fibro calcified plaque covering almost 270 degree with a plaque burden of 58% and MLA = 3.86 MM square DES: 4*13 MM At 10 ATM Post-dilatation done with 4.5*8 MM NC balloon at 15 ATM Post-stenting IVUS pull back done Post-stenting IVUS showed good apposition with proper expansion of stent 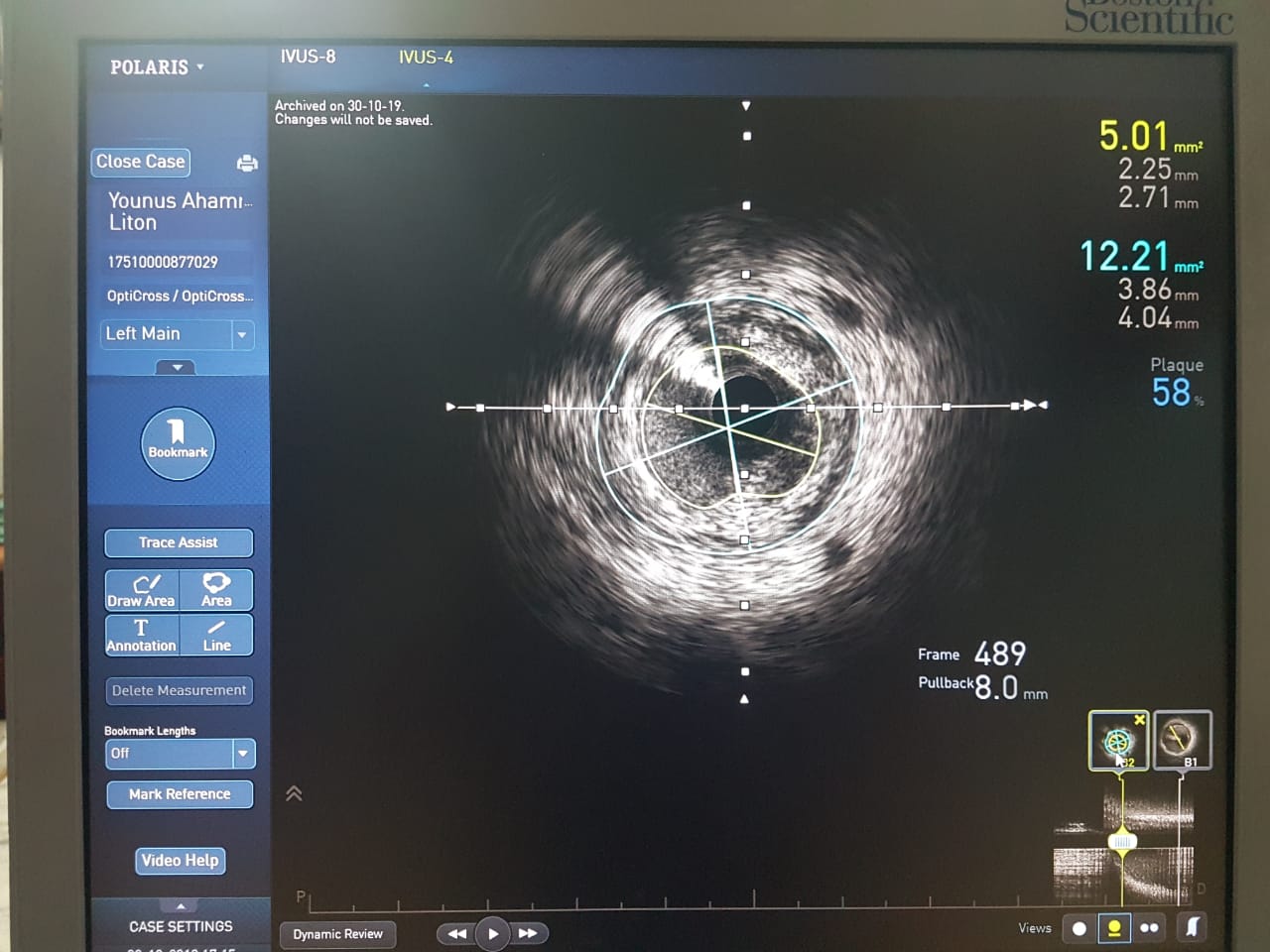 - Case Summary:
LM disease when detected during angiography is usually managed through heart team for discussion / decision. However in unstable patient with recurrent symptoms or in patients where CABG is not possible, Adhoc PTCA stenting with IVUS study to be done. IVUS helps in decision making for pre-PCI strategy. Proper stent sizing and stent apposition with respect to achieving MLA is better achieved with IVUS. |
|