Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191112_005
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Wide Angle LM Bifurcation Lesion: Difficulty and Strategy | |
| Sheng Yun Wang1 | |
| Changhua Christian Hospital, Taiwan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
61 y/o male
-Relevant clinical history and physical exam:
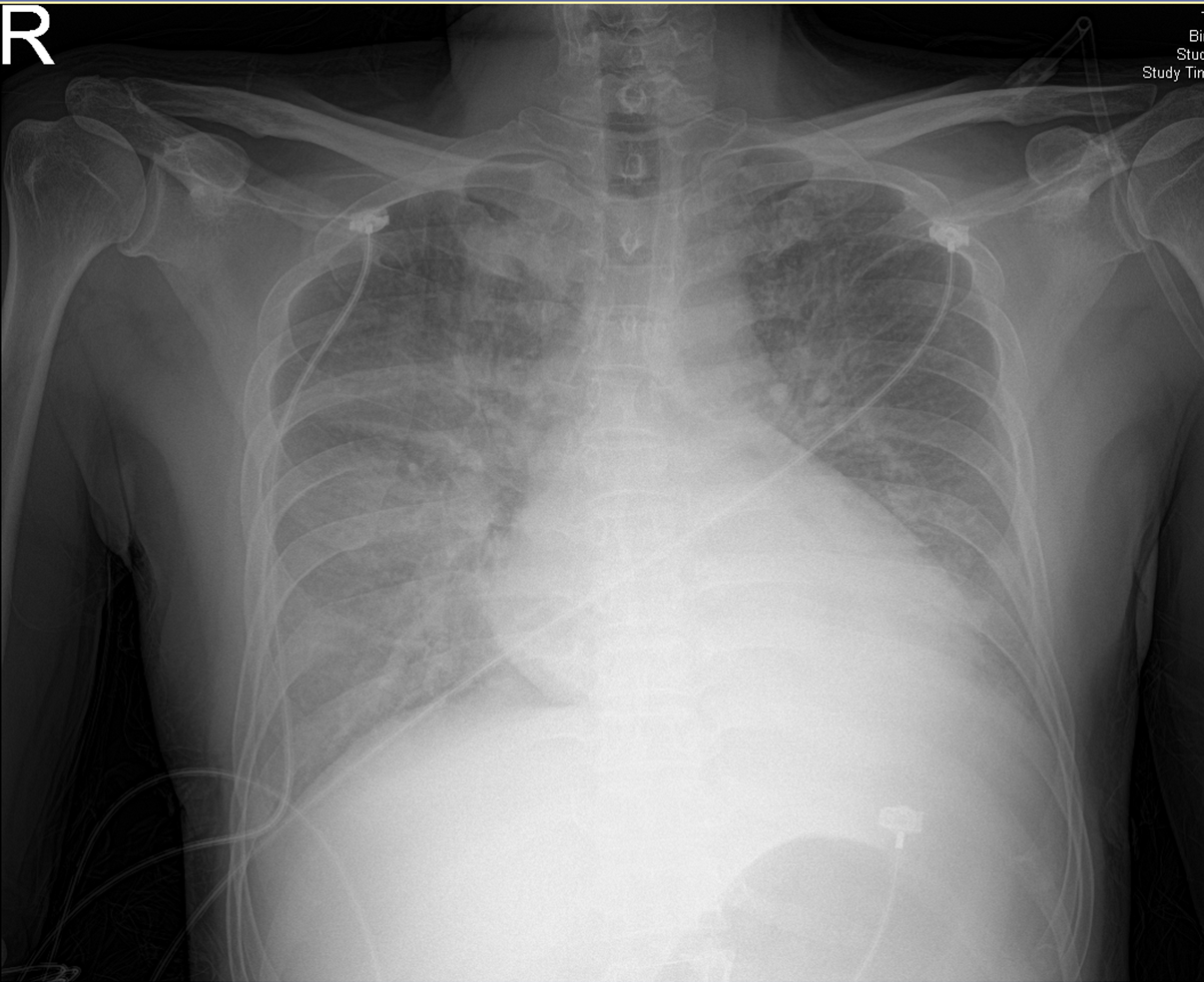
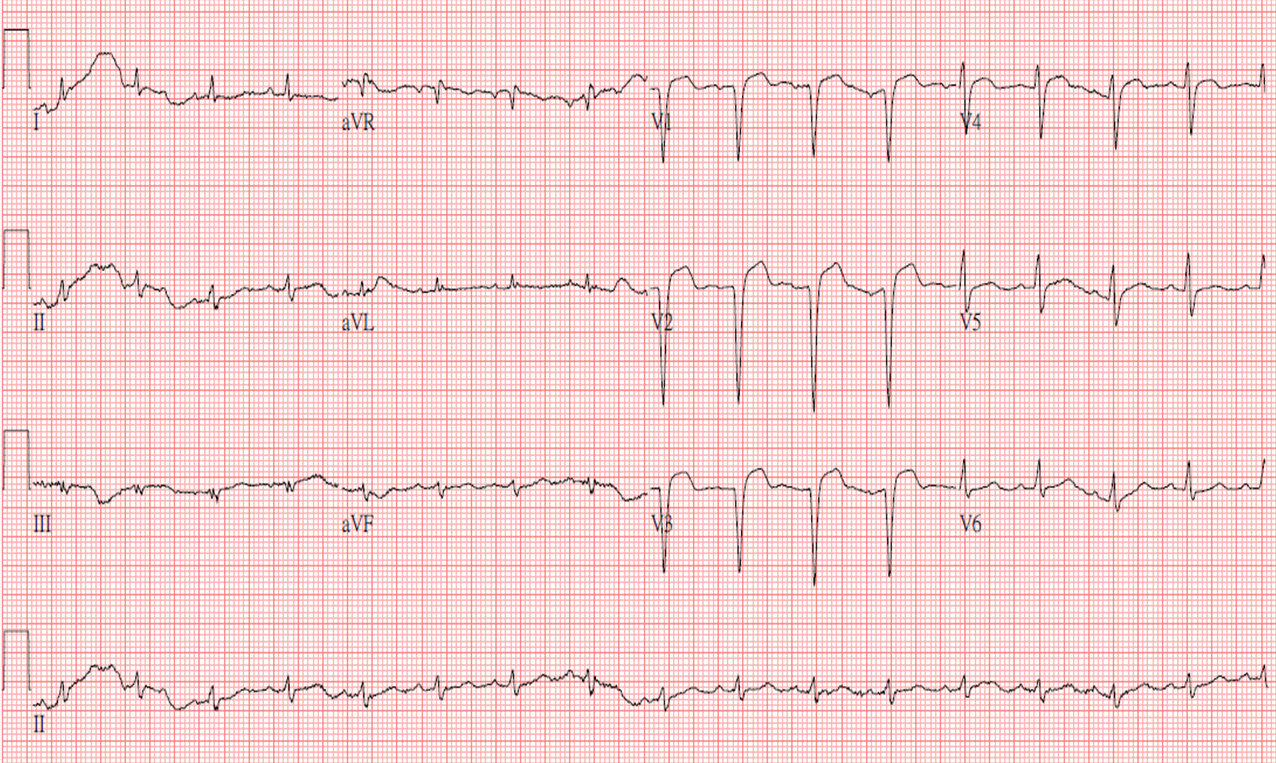
With history of hypertension, type 2 DM, present dyspnea 2 days, visited emergency department. PE showed bilateral rales, shallow respiratory pattern. Lab data showed elevated cardiac enzyme, chest x ray showed pulmonary edema, ECG showed V1~V3 QS pattern, ST elevation, echocardiography showed almost diffuse hypokinesia.
-Relevant test results prior to catheterization:
ECG showed V1~V3 QS pattern, ST elevation.CXR showed pulmonary edema.
  - Relevant catheterization findings:
RCA: atherosclerosisLCA: LM bifurcation lesion, medina 1,1,1 lesion, wide angle between LAD and LCx coronary artery, Middle LAD severe stenosis, distal LCx severe stenosis.CAD-2VD with LM bifurcation lesion, LAD-m, LCx-d lesion c/w ACS with NSTEMI.
|
|
|
[Interventional Management]
- Procedural step:
We applied Rinato wire to distal LAD via Launcher AL1.5/ 7Fr. Guiding catheter, Runrhtough floppy wire to distal LCX. Pre-dilate with Sapphire 2.5/15mm inflated up to 8ATM for mid LAD, Tried to push balloon to LCX, but wire twisted, withdrew with Runthrough floppy wire, tried to rewire, but failed. Added on Sion wire, successfully applied to distal LCX. Predilate with Sapphire 2.5/15mm inflated up to 8ATM for mid LCX => IVUS for lesion optimization, mid LAD :3.0mm, proximal LAD 4.0mm, LM:4.5-5.0mm, (failed to pass IVUS to distal LCX via Sion wire, exchange to ACS Extrasupport wire) ostial LCX 3.0-3.5mmThen CAG showed mid LAD Type C dissection, Stent deployment for mid LAD with Orsiro 3.0/40mm inflated up to 8ATM. We used Mini-crush technique for LM-LAD-LCX lesion, stent deploy with Orsiro 3.0/13mm inflated up to 10ATM for ostial LCX. Stent deploy and crush LCX stent with Resolute Onyx 4.0/34mm inflated up to 12ATM for LM-LAD. But difficult advance the LCx stent to ideal position. Rewire with Fielder FC to LCX with Stride MC, then exchange to Hi Torque Whisper Extra Support wire, and successfully advance the LCx stent, then inflated stent and perform the Mini-crush. Post dilatation and kissing balloon dilatation for LAD with stent balloon 4.0/34mm up to 14ATM, LCX with NC Euphora 3.0/8mm upt o 8ATM, post-dilate with NC Euphora 3.0/8mm inflated up to 20ATM => CAG showed residual stenosis <10%, TIMI 3 antegrade flow.
- Case Summary:
In this wide angle LM bifurcation lesion, it is difficult to plan the strategy. We applied the Mini-crush technique for the patient due to that LCx territory is wide and its diameter still had discrepancy with LAD. So we need to preserve it, it is difficult to advance the wire, IVUS, stent depolyment due to large and sharp angle. We increased support and finally advanced the stent, successful Mini-crush technique. In a double stent strategy for the wide and large angle bifurcation lesion, Mini-crush technique was acceptable and maybe consider.
|
|