Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191112_004
| CORONARY - Chronic Total Occlusion | |
| Successful REWIPE (REtrograde Wiring into Antegrade PEnetration Catheter) Technique for RCA CTO Lesion | |
| Sheng-Wei Huang1, Chun Hung Su1, Shih-Chi Liu2 | |
| Chung Shan Medical University Hospital, Taiwan1, Fu Jen Catholic University Hospital, Taiwan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr. Tsai
-Relevant clinical history and physical exam:
This is a 50 years old man, a heavy tobacco smoker. He received medication treatment for hypertension and hyperlipidemia for more than 5 years. He presented with intermittent chest tightness on and off in recent two years and it deteriorated gradually. Coronary angiography performed 4 month ago disclosed multi-vessel disease. After PCI for LAD, staged PCI for RCA this time was arranged. Physical examination revealed clear heart sound and no pitting edema.
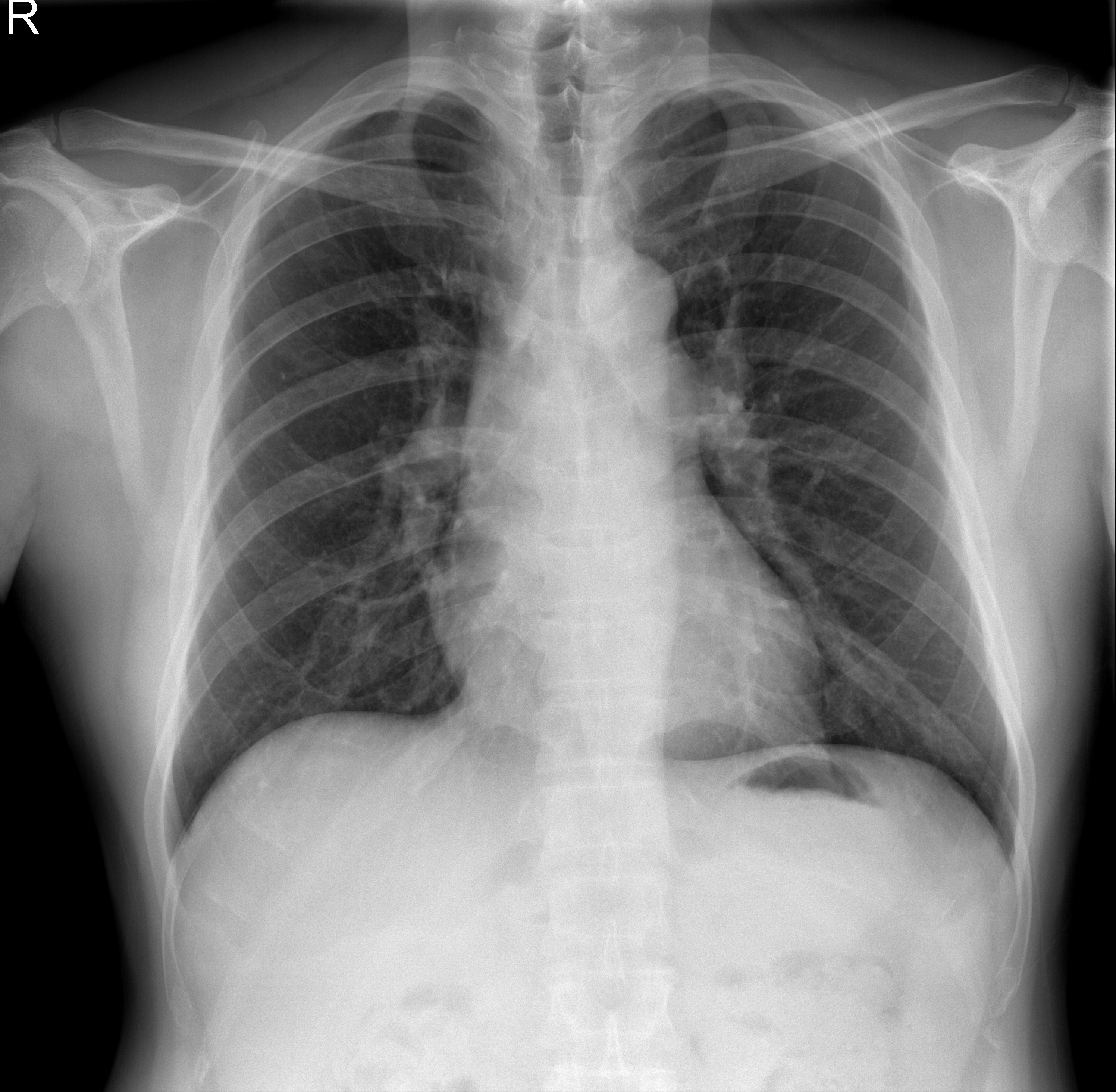
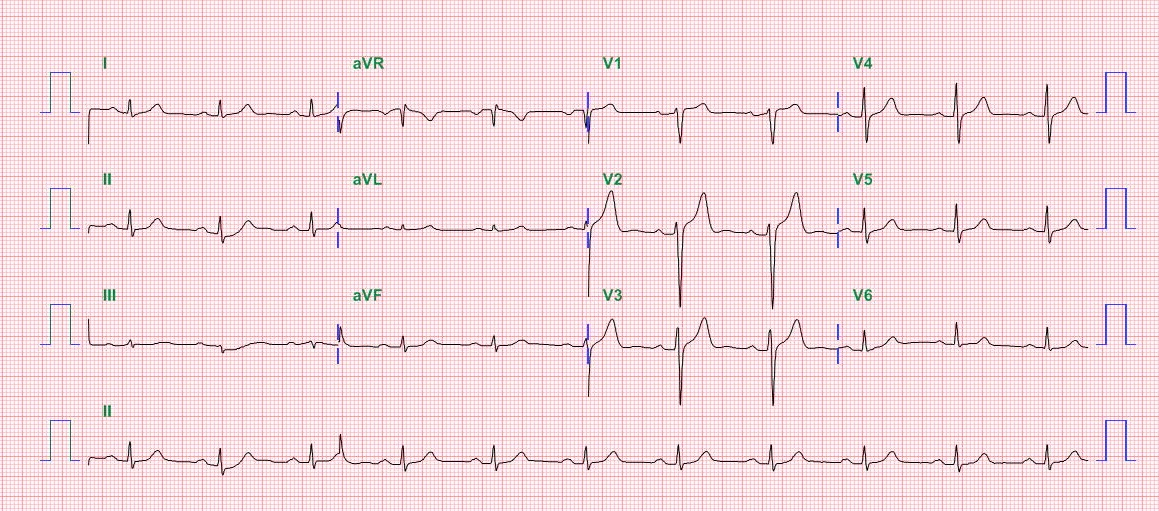 -Relevant test results prior to catheterization:
An echocardiogram demonstrates systolic dysfunction, mild mitral regurgitation, a dilated left atrium, and an ejection fraction (EF) of 59%.
 - Relevant catheterization findings:
Angiography reveals patent left main and proximal to middle Left anterior descending artery stent. Distal Left circumflex has 40% stenosis. Right coronary artery: M-RCA TO D-RCA chronic total occlusion with class II collateral from LAD epicardial branch. The collateral is corkscrew, hair-pin bended channel into distal RCA. The stump was blunt and the occlusion length is more than 20 mm with little calcified. J-CTO score = 2.
|
|
|
[Interventional Management]
- Procedural step:
LCA was cannulized with EBU 3.5 Guiding catheter. RCA was cannulized with AL 1. RCA ostium dissection was noted and we used REBEL 4.5*24mm directly stenting and post dilated by 5.0 * 20 mm NC EMERGE up to 20 bars. Antegrade PCI was preformed first with FineCross microcatheter. We advanced Sion (for Finecross) and then tried Gaia 3 and then Conquest Pro12 and Gaia 1 alternately and finally went through proximal cap to D-RCA but could not puncture into distal true lumen (under contralateral injection). We left Conquest Pro 12 within another antegrade Stride microcatheter. We tried retrograde, we advanced Sion till D-LAD epicardial collateral with Finecross 150 then used Sion with broken tip and then Sion black to D-RCA CTO distal cap and then tried puncture with UB3 and then another Conquest Pro 12 and these wires all stop at distal cap. Then antegrade Conquest Pro 12 successfully kisses retrograde wire so Reverse-CART was planned first. We have failed to advance the 1.0 mm balloon and the antegrade wire was accidently pulled back. We tried re-wiring and used Fielder FC with Stride 2.2 Fr antegradely. Then Retrograde wire (Conquest Pro 12) successful passed through CTO lesions and into antegrade stride and then into antegrade guiding. (REWIPE) We advanced OTW 1.5 * 15 mm balloon into retrograde wire (in antegrade guiding) and advanced through the CTO lesions. After serial POBA and two XIENCE stent deployment, angiography showed TIMI 3 flow.
- Case Summary:
Guide catheter-induced dissection of the coronary arteries is an uncommon but potentially catastrophic complication. Even though the AL 1 Guide catheter do much more than JR we still need the good support to complete successful CTO-PCI.
Special wires such as Broken-tip Sion may require for small, corkscrew-like collateral channel tracking. Re-wipe is an alternative technique other than externalization of wire, Re-wipe can complete CTO-PCI procedure and minimize collateral vessel damage, especially in such tortuous and hair-pin collateral vessel. Re-wipe and Intracoronary Rendezvous technique can provide additional extra-support and reduce donor or collateral vessel injury. |
|