Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191112_003
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Transradial Percutaneous Coronary Intervention to Treat Bifurcation Lesions in Acute Left Main Artery Myocardial Infarction by Using Sheathless Guiding Catheter | |
| Yao-Tsung Chuang1, Chien Hsien Lo2 | |
| Chung Shan Medical University Hospital, Taiwan1, Da-Chien General Hospital, Taiwan2, | |
|
[Clinical Information]
- Patient initials or identifier number:
52 years old female patient
-Relevant clinical history and physical exam:
Denied DM Denied HTN Smoking 1PPD for 30 years Denied chronic jideny disease Denied hyperlipidemia Physical examination Regular heart beats Diffuse rales breathing sound Visiting ER because of severe chest ain and cold sweating Low blood pressure was noted bp: 90/60 mmHg -Relevant test results prior to catheterization:
Chest X ray: cardiomegaly ; acute pulmonary edema EKG: sinus rhythm; AVR st elevation; diffuse ST depression and T inversion H.S troponin I: 716.6 pg/dl CPK:62IU/L; CK-MB:5.8ng/mL 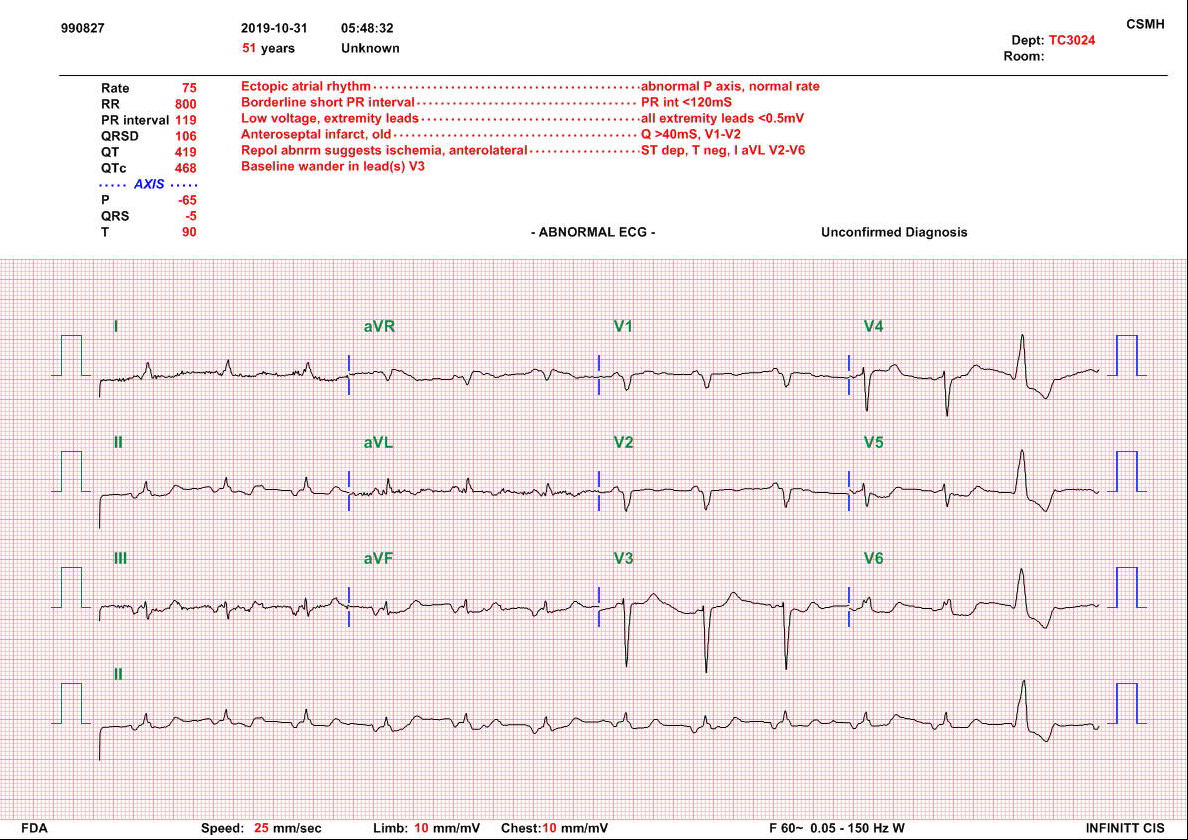 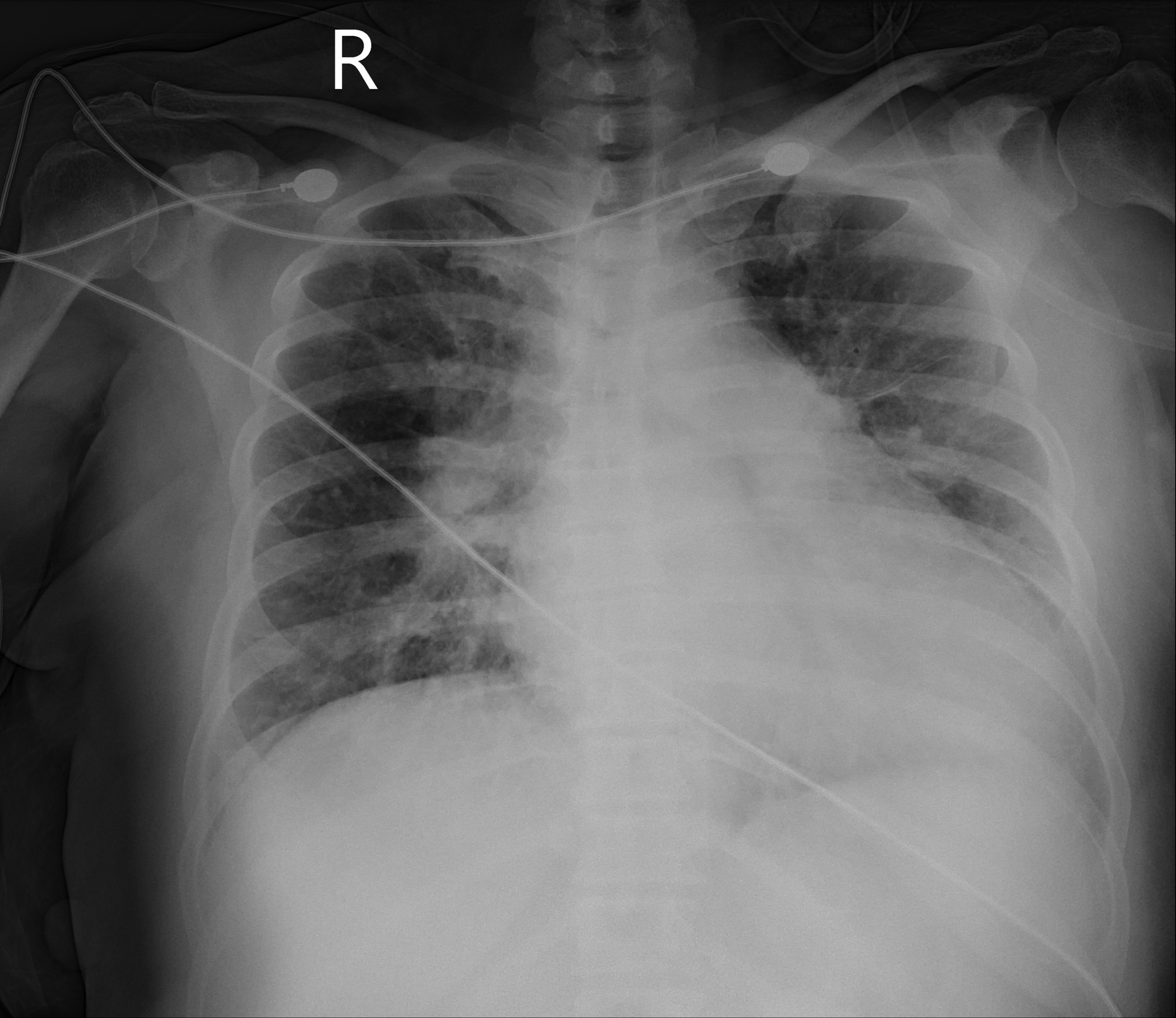 - Relevant catheterization findings:
Fisrt CAG: LM total occlusion RCA: distal RCA 100% stenosis ; collateral artery frome RV branch to D-RCA second CAG after 4 days LM: d-LM:90% stenosis LAD: LAD-OS:90% stenosis; diffuse lad dissection LCX: LCX-OS:90% stenosis RCA: distal RCA 100% stenosis; collateral artery from RV branch to D-RCA |
|
|
[Interventional Management]
- Procedural step:
First PCI1.Cannulated by EBU 7 Fr guiding catheter2. Sion wire to LAD and floppy to D1.3. P-LAD was dilated by a 2.5x15 mm Trek with maximal 10atms.4. Cardiogenic shock was noted; intubation was done, CPR for 5 minutes ECMO and IABP support were given, and ICU admission.5. Hemodynamic status stable under V-A ECMO and IABP support
Second PCI (4 days later)1. Left main artery was engaged by EBU 7 Fr guiding catheter (Sheathless from right transradial artery; right femoral artery: ECMO A site; left femoral artery: IABP)2. We use Sion, Fielder FC, XTR and Gaia2 wires to diatal LAD , but failed (long dissection lesion )3. A Sion wire to LAD-D1 and Floppy wire to LCX4. DK crush technique for LM bifurcation lesion (3.5x23mm Xience in LM-LAD and 3.0x23mm Xience X in LCX)5. TIMI I flow ofD-LAD - Case Summary:
1. LM AMI is a critical condition. 2. IABP and ECMO support before LM primary PCI are indictaed. 3 Transradial Sheathless guiding catheter technique is useful for two stent technique. 4. Long dissection lesion is difficult to pass wire. 5.Complete revascularization is considered for this patient. |
|