Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191110_003
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| DK Crush for Bifurcation Lesion in STEMI Setting | |
| S M Mamun Iqbal1 | |
| M. H. Samorita Hospital and Medical College, Bangladesh1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr S B
-Relevant clinical history and physical exam:
Mr S B, a-40-year-old gentleman presented in ER with compressive central chest discomfort. He had no previous history of angina. He was a smoker, non-hypertensive and non-diabetic. On physical examination, he was haemodynamically stable and there was no sign of heart failure.
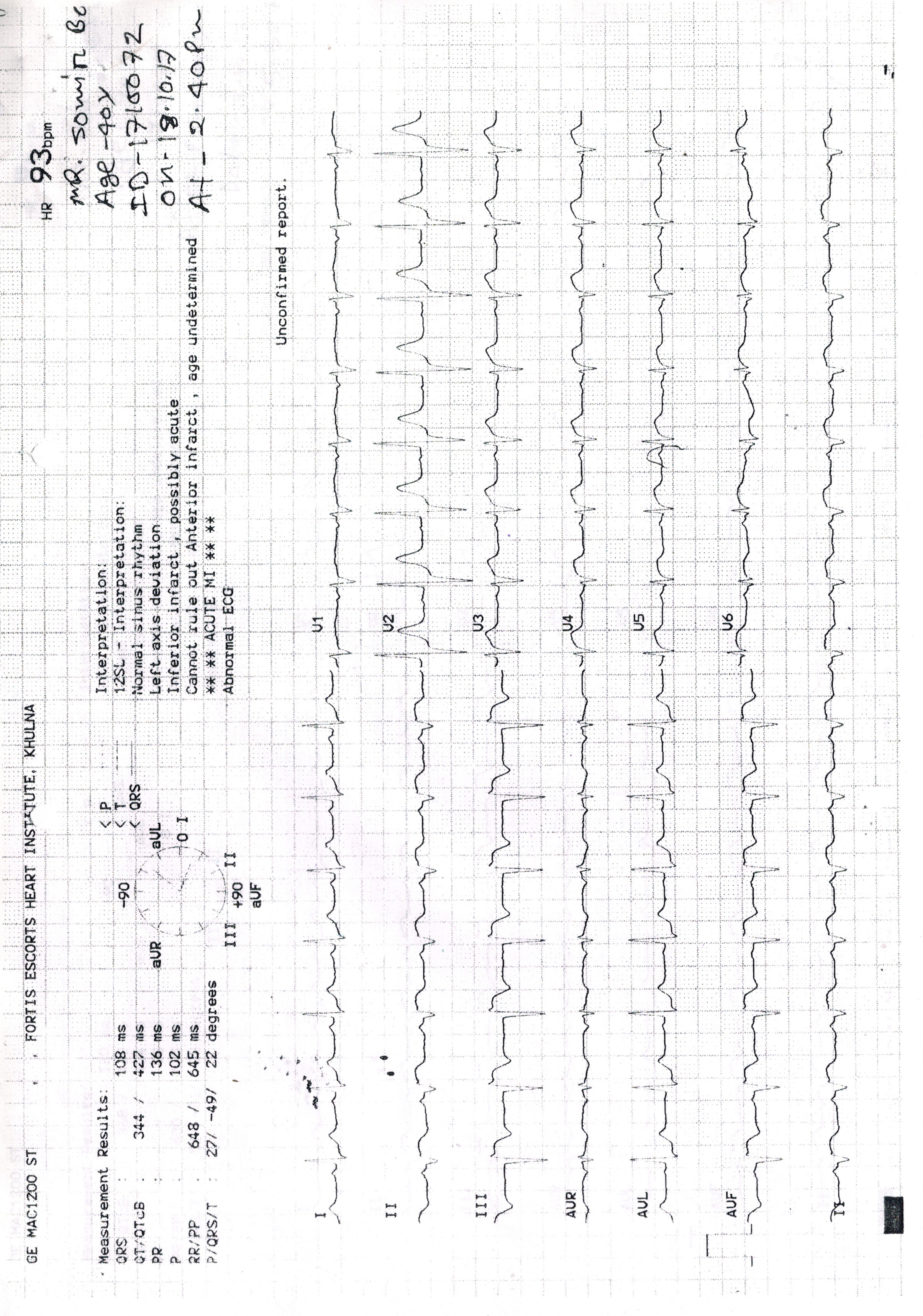
-Relevant test results prior to catheterization:
Troponin I - RaisedSerum creatinine- 1.6 mg/dlECG- ST elevation in II, III, avF, V4-6; pathological Q in II, III, aVF ; ST depression in I, aVL; Tall R in V2; Poor R wave progression up to V4.Bedside Echocardiography - The inferior, posterior and lateral walls are severely hypokinetic. The anteroseptum and apex are mildly hypokinetic.
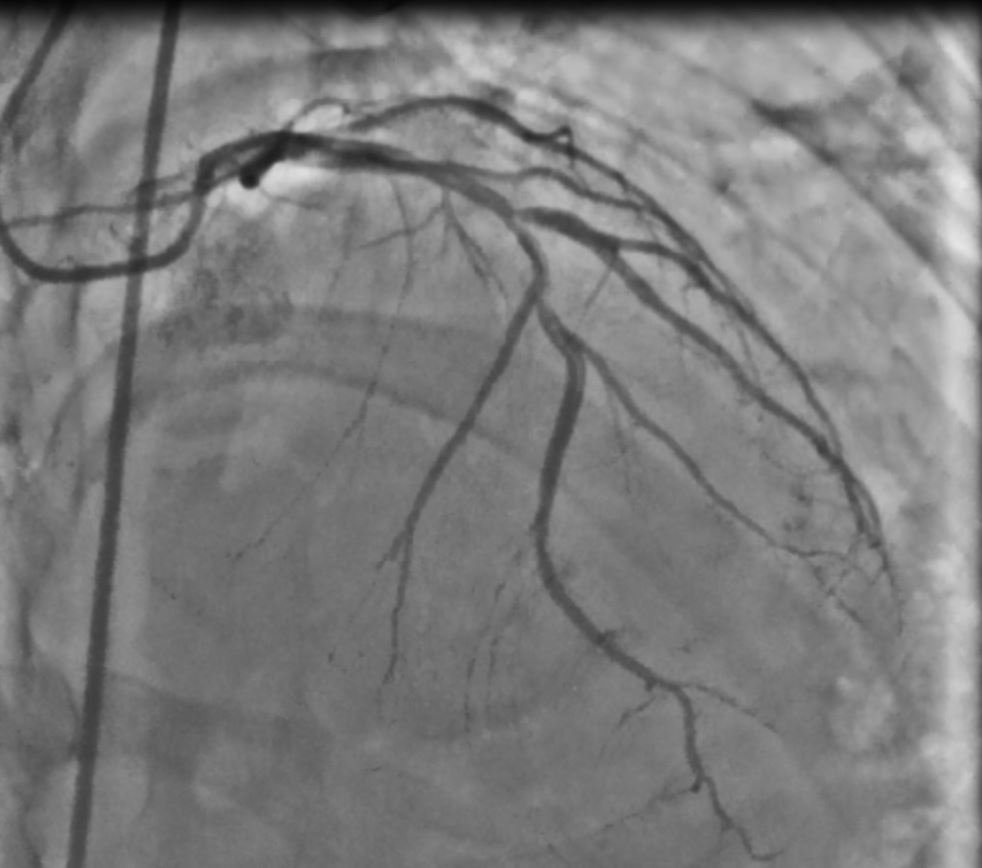
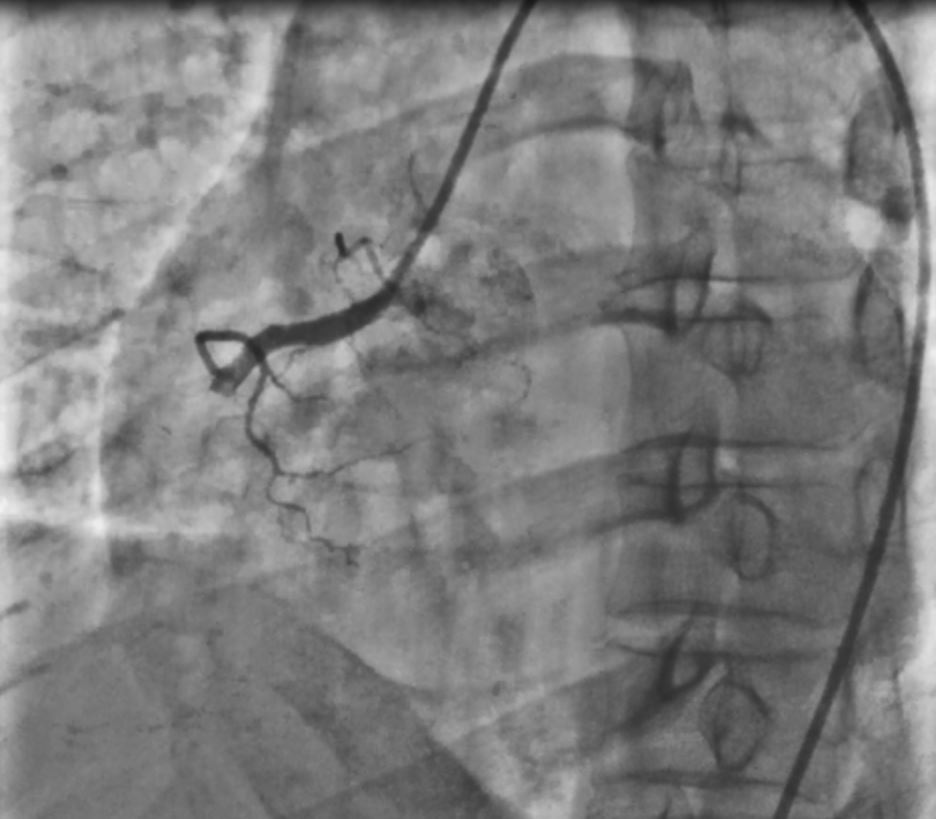
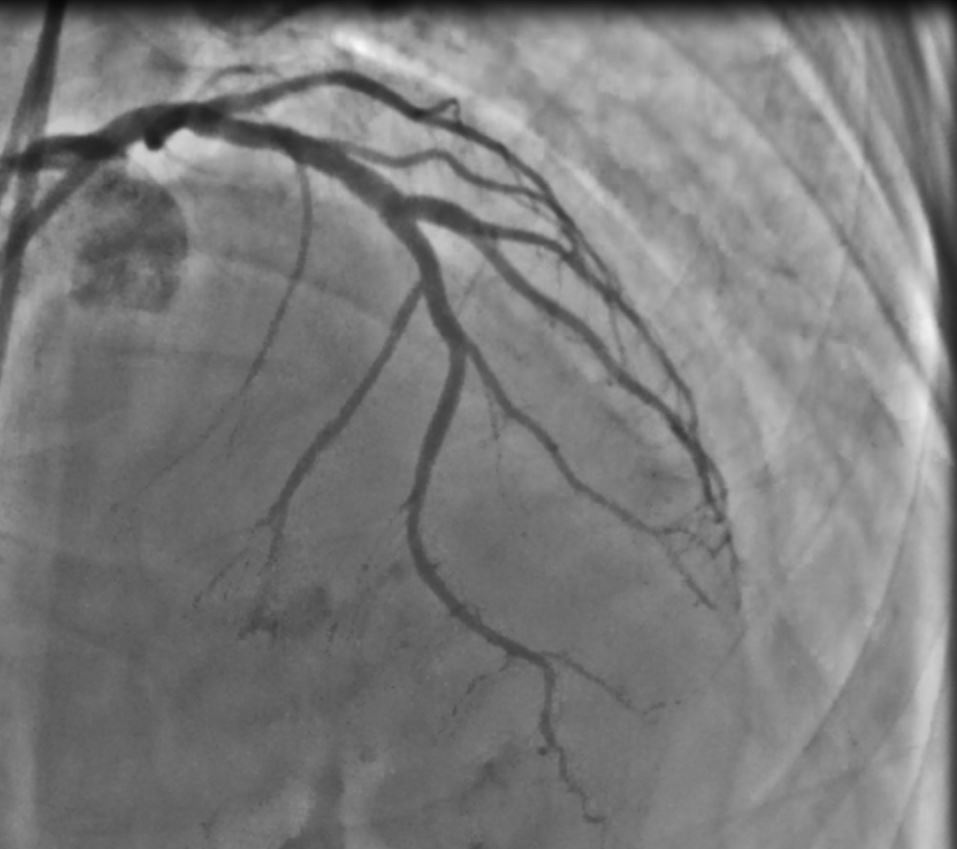
 - Relevant catheterization findings:
Our clinical diagnosis was STEMI- Inferior with posterolateral extension. With the aim of primary PCI, we did coronary angiogram which revealed-Left main- Disease freeLAD - Type III with Medina I,I,I bifurcation lesion involving proximal to mid LAD and Diagonal ostium.LCX - Non dominant, small vessel. Disease free.RCA - Dominant with a thrombus containing total occlusion in proximal part.
  |
|
|
[Interventional Management]
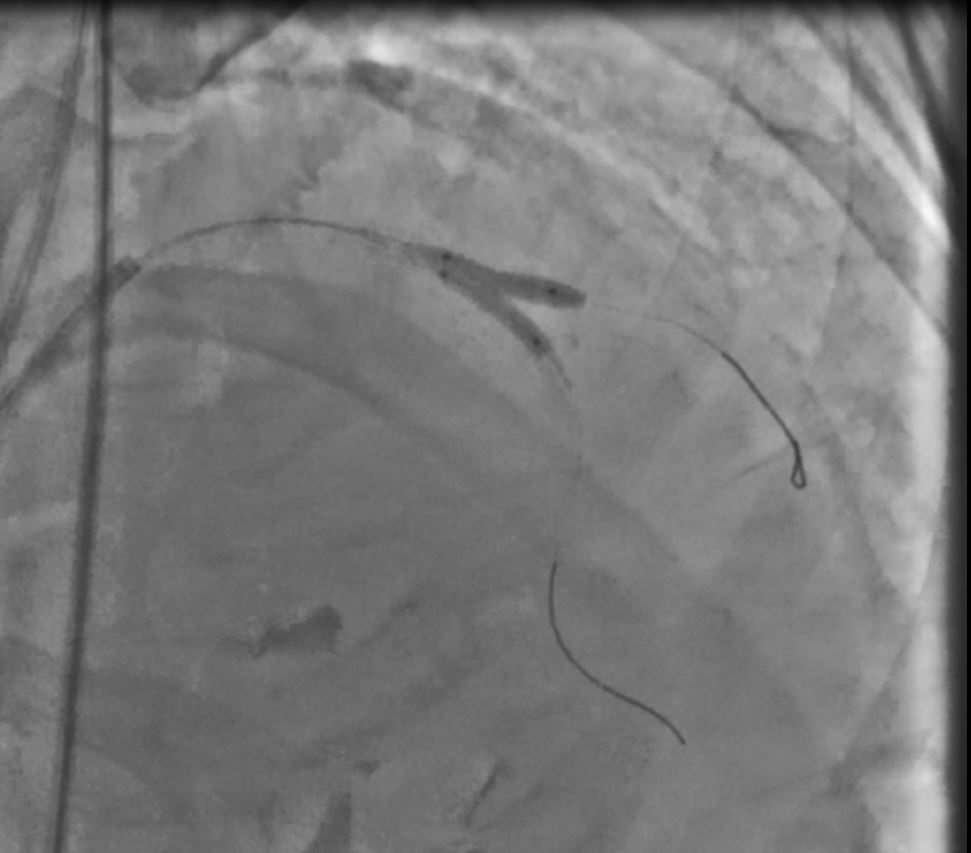
- Procedural step:
Primary PCI to RCA was done with a 3.5 X 28 mm Cobalt chromium BMS. The patient recovered well and was readmitted for staged PCI of the LAD bifurcation 2 weeks later. Through right femoral artery, a 7 Fr XB 3.0 guide catheter was passed to engage left main artery. Two 0.014 inch 190 cm BMW wires were crossed through LAD and diagonal lesions. Predilatation of diagonal and LAD were done with 2.0 X10 mm and 2.0 X 15 mm NC balloons respectively at 10 ATM. A 3.5 X 12 mm Everolimus DES was deployed at ostioproximal part of diagonal at 12 ATM, keeping 2 mm of stent in LAD. The wire and balloon were removed from diagonal. The proximal edge of the stent was crushed with a 3.0 X 15 mm NC balloon placed in LAD at 14 ATM ( 1st crush). The stent was recrossed with BMW wire and first kissing balloon dilatation was done with a 3.5 X 15 mm NC balloon in Diagonal and 3.0 X 15 mm NC balloon in LAD, inflated at 10 ATM. Again, the wire and balloon were removed from diagonal. A 3.0 X 32 mm Everolimus DES was deployed in LAD at 12 ATM crushing the diagonal stent ( 2nd crush). Proximal optimization (POT) was done with 3.5 X15 mm NC balloon at 12 ATM. A BMW wire was recrossed into diagonal stent and a second kissing balloon inflation was done with 3.5 X 15 mm NC balloon in diagonal and 3.0 X 15 mm NC balloon in LAD, inflated at 12 ATM. Final POT was done with a 4.0 X 15 mm NC balloon at 16 ATM. Final angiogram showed the LAD and diagonal were optimally revascularized with TIMI- III distal flow.
   - Case Summary:
Although the current guidelines permit revascularization of non-IRA lesions before hospital discharge (class II A), considering the renal impairment and the complexity of the LAD lesion, we decided to do the DK crush after two weeks of primary PCI with satisfactory outcomes.
|
|