Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191109_001
| CORONARY - Acute Coronary Syndromes (STEMI, NSTE-ACS) | |
| Primary PCI to Total Left Main Occlusion as a Bridging Therapy in STEMI with Rapidly Deteriorating Cardiogenic Shock in an Undiagnosed Aortic Dissection Type A | |
| Wongwaris Aphijirawat1 | |
| Queen Sirikit Naval Hospital, Thailand1, | |
|
[Clinical Information]
- Patient initials or identifier number:
Mr.ST
-Relevant clinical history and physical exam:
Case 35-year-old male not known underlying disease
-Relevant test results prior to catheterization:
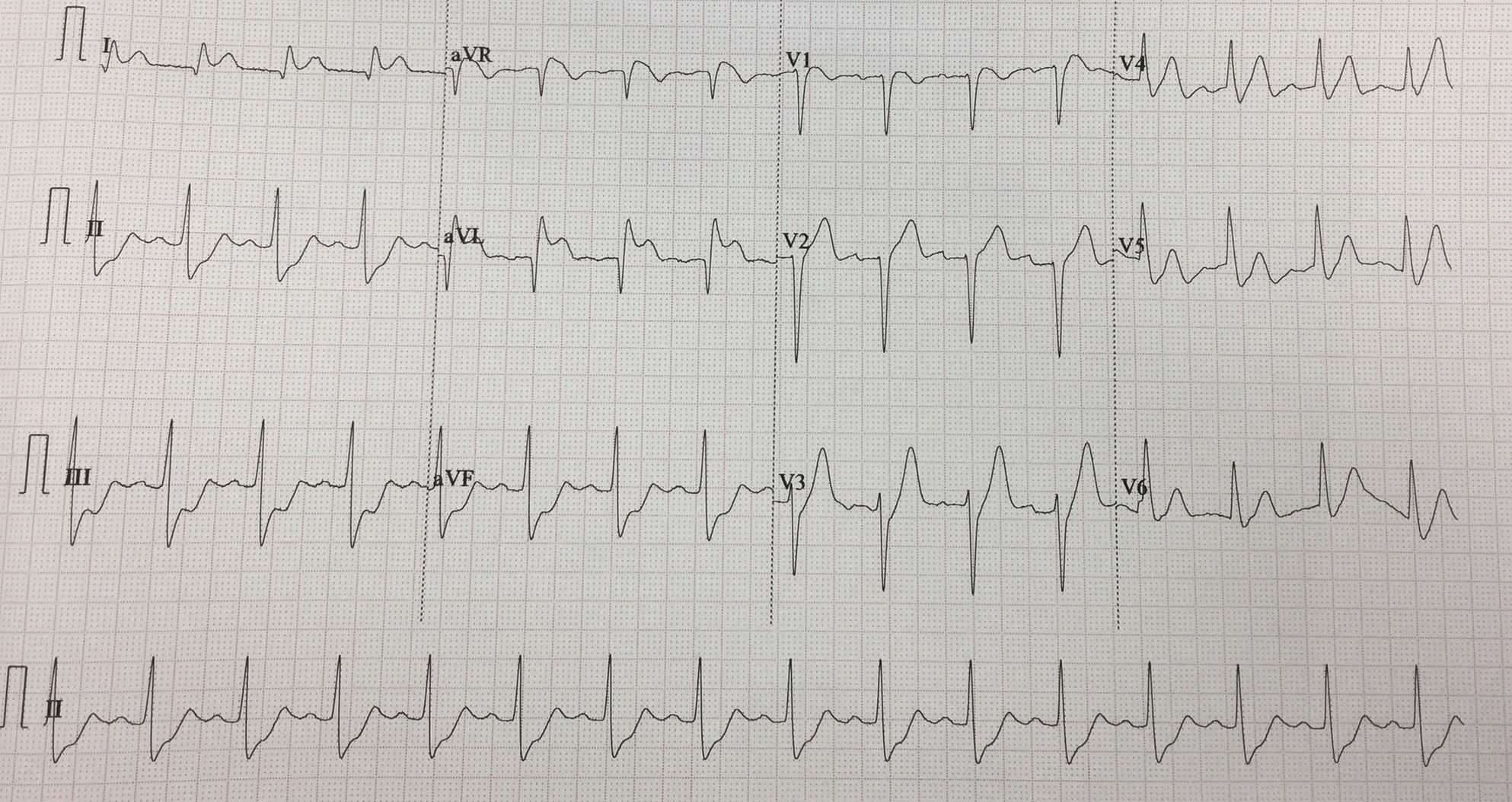
ECG showed NSR with ST elevation at I,avL , avR with ST depression in II, III, avF and poor R wave progression
 - Relevant catheterization findings:
CAG: Dominant RCA vessel with free of stenosis
Note: The patient was markedly tachypnea and very agitation at cath lab, many of sedative drug and intubation were done. |
|
|
[Interventional Management]
- Procedural step:
6F sheath was inserted via right femoral artery and IABP was inserted via Left femoral artery6F JL 4.0 catheter was engaged to Left coronary arteryA 0.014 Whisper wire and 1.8Fr Finecross MG microcatheter was passed through the left main, tip injection was confirmed the true lumen of LCx.A 2.0 x12 mm and 2.5 x15 mm Mini Trek balloon was predilated at ostial to proximal left main artery up to 14 atm.Integrilin 6.2 mg and prasugrel (10 mg) 6 tabs were given.A 3.0 x 16 mm Firebird II and 3.0 x14 mm Biofreedom couldn't pass the ostial left main for multiple attempts, so 2.0 x15 mm NC Sprinter balloon was used to predilate the LM lesion up to 16 atm.Again, 3.5 x 14 mm Biofreedom stent was unable to cross the left main lesion despite buddy wire technique was used. At this time, the patient developed severe hypotension and large amount of pink frothy sputum came out from endotracheal tube. Patient was very agitated and tried to pull the tube off, multiple doses of midazolam and fentanyl were given IV.6F EBU guiding was exchanged with JL4.0 for extra support.A 3.0 x15 mm NC balloon was predilated to the Left main lesion again, this time 4.0x11 mm Biofreedom stent could pass the lesion and deployed at the ostial to proximal left main artery.Final angiogram showed TIMI III flow in LCx , TIMI I in LAD. When we reviewed the angiogram, there was moderate to severe aortic regurgitation. We performed the echocardiogram and showed aortic dissection Sanford type A, CVT was call for emergency operation.
- Case Summary:
This case, patient was unstable to go to surgery at the first presentation due to acute pulmonary edema with cardiogenic shock and also, we did not perform echocardiogram at emergency room because STEMI fast track was activated.In undiagnosed Type A aortic dissection causing total left main occlusion resulted in rapidly deteriorate cardiogenic shock, PCI to left main maybe used as an bridging therapy while awaiting for definitive surgery.
|
|