Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191108_001
| CORONARY - Complex and Higher Risk Procedures for Indicated Patients (CHIP) | |
| Tag Team - Simultaneous Bifurcation and CTO Disease Intervention | |
| Wan Faizal Wan Rahimi Shah1, Jayakhanthan Kolanthaivelu2, Kumara Gurupparan Ganesan3 | |
| Cardiac Vascular Sentral Kuala Lumpur (CVSKL), Malaysia1, Cardiovascular Sentral Kuala Lumpur, Malaysia2, National Heart Institute, Malaysia3, | |
|
[Clinical Information]
- Patient initials or identifier number:
A.M
-Relevant clinical history and physical exam:
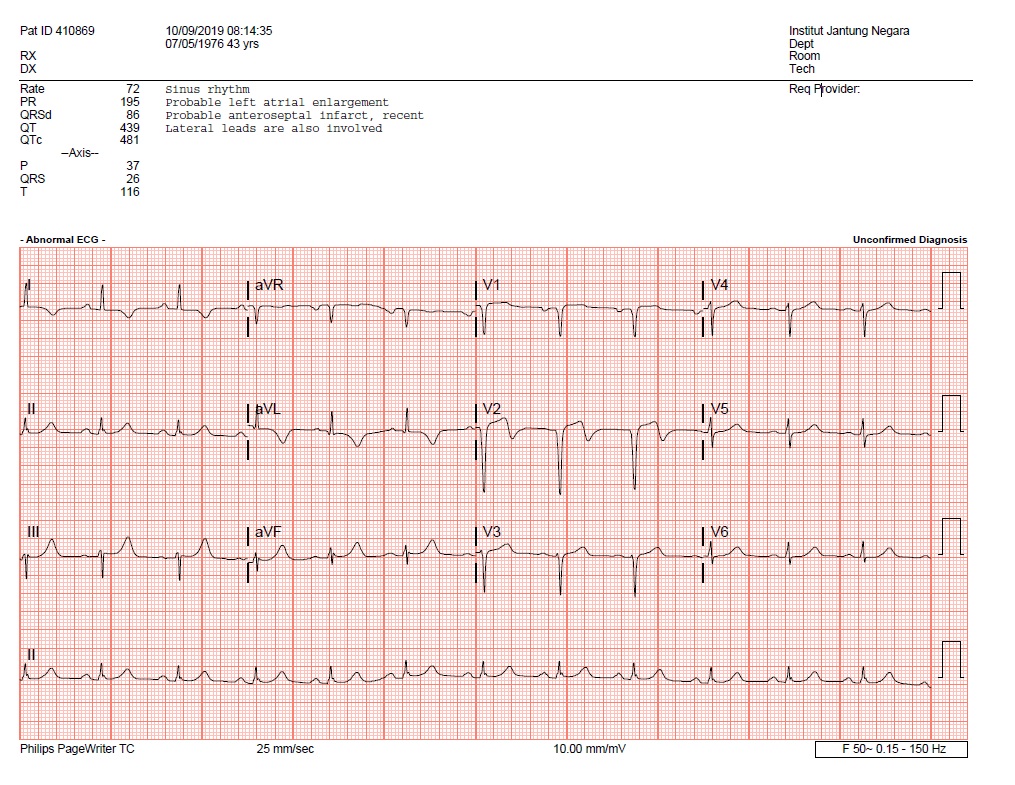
A young 43 years old male was referred to our institute for further intervention. He had underlying obesity, diabetes mellitus, hypertension and dyslipidemia. He is an active smoker. He presented one month earlier in a non-PCI capable hospital for atypical right sided chest pain. ECG done had already shown established Anteroseptal MI. He was referred to us for further cardiac assessment, KIV for Coronary Angiogram.
-Relevant test results prior to catheterization:
Echocardiogram from referring centre showed LVEF of 41% with hypokinesia in the basal and mid anterior/anteroseptal walls. No other significant valvular disease was seen.Chest X-ray showed borderline cardiomegaly with no evidence of any pulmonary congestion.ECG done in our centre showed Q waves in leads V1-V2.
  - Relevant catheterization findings:
Our initial Coronary Angiogram findings were as below
LMS - normalLAD - CTO with tapered entry, calcification within CTO lesion- proper dual injection done showed occlusion segment was short with calculated J-CTO score of 1LCx - severe mid segment disease, subtotal occlusion of OM1, moderate-severe disease OM2RCA - dominant vessel with ectatic architecture and mild scattered disease He was counselled on table on intervention. He was strongly keen to proceed with PCI as oppose to bypass surgery, 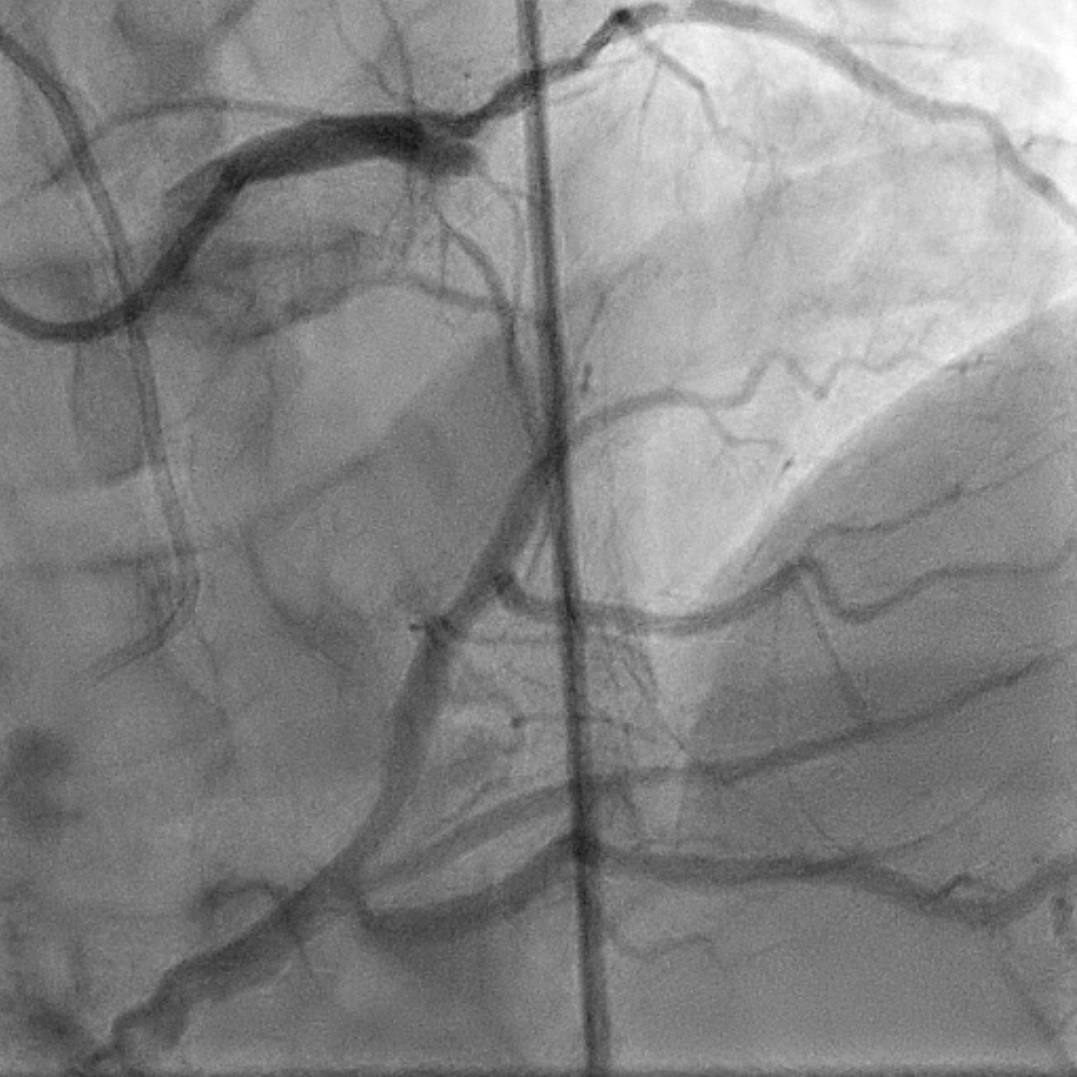 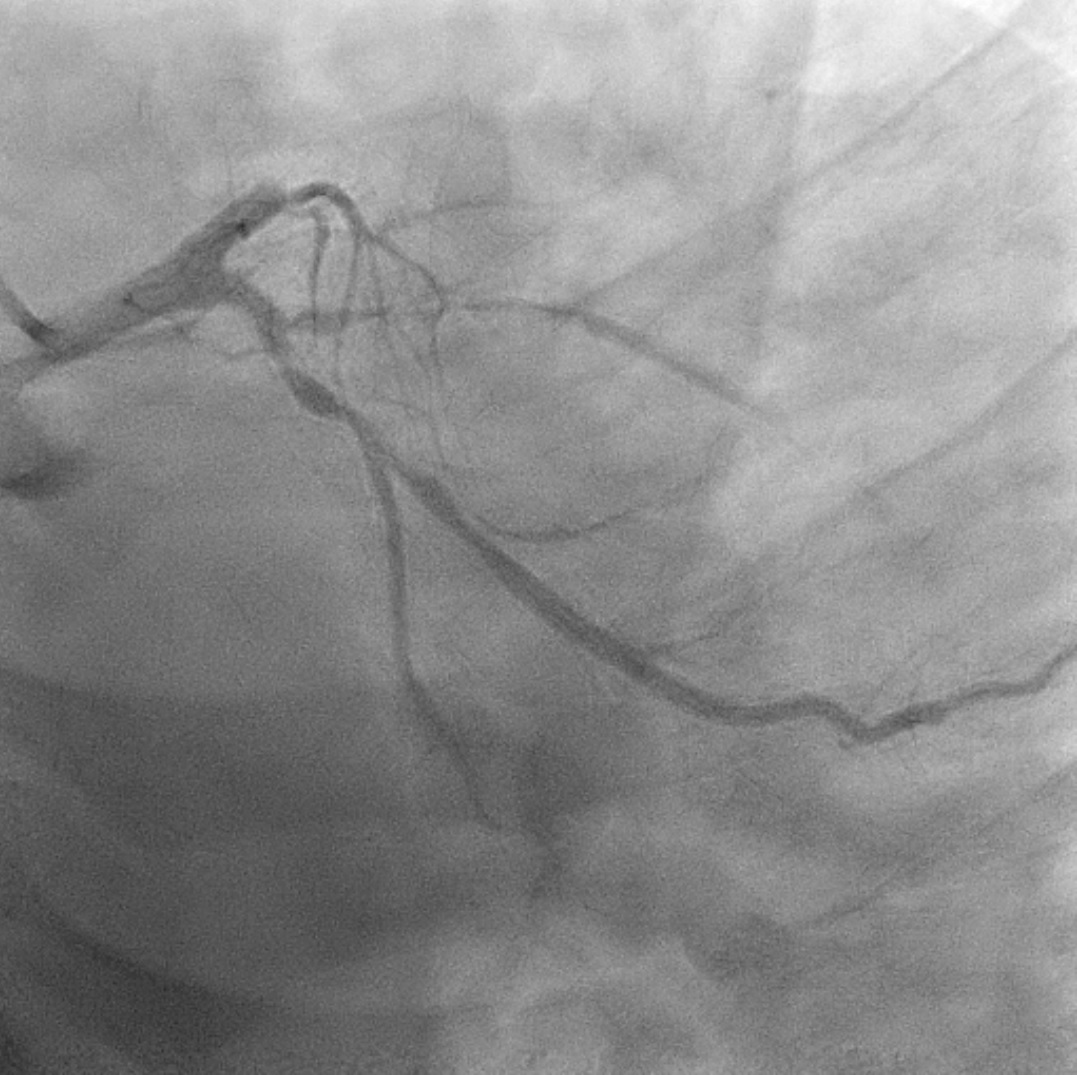 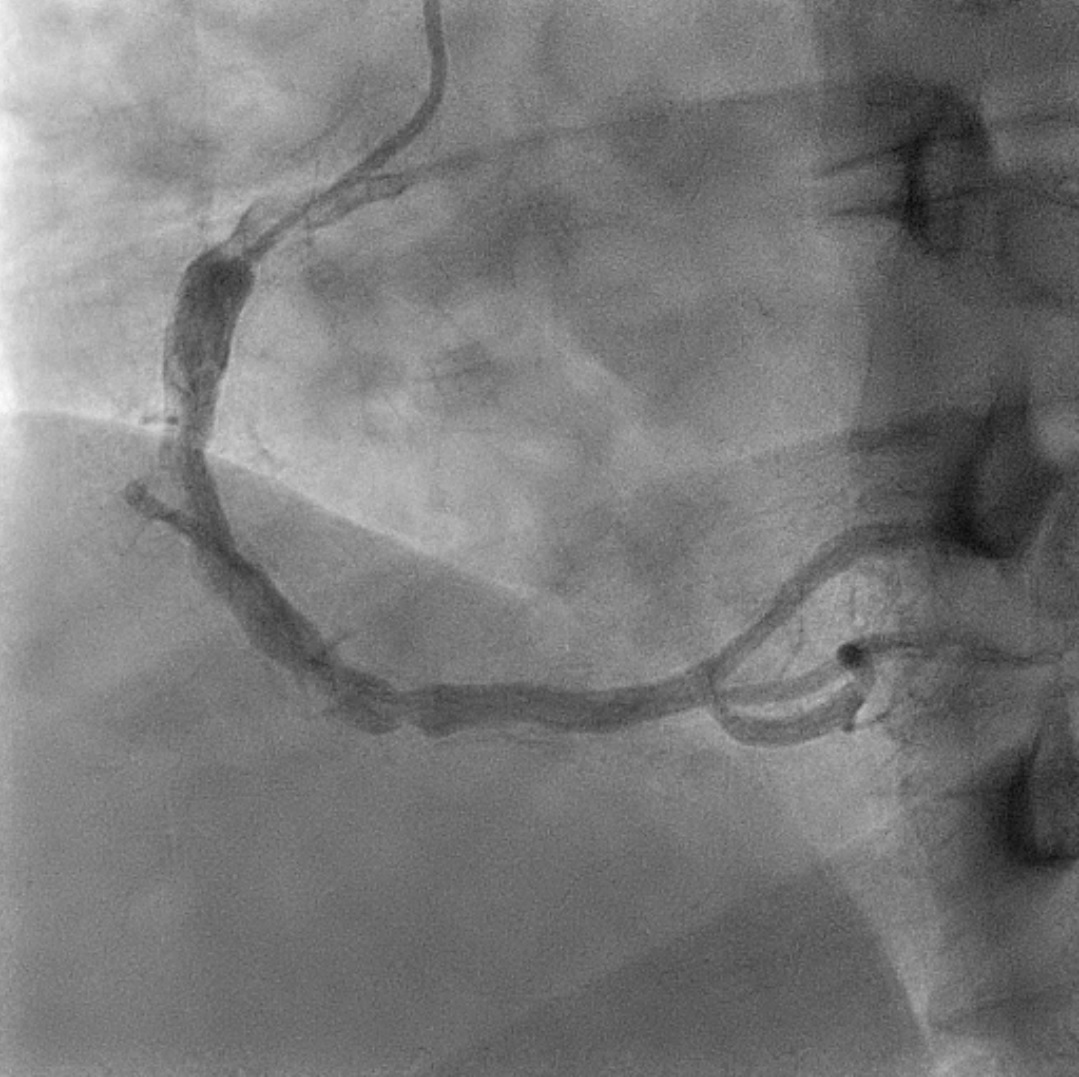 |
|
|
[Interventional Management]
- Procedural step:
6Fr EBU 3.5 guiding catheter used via right femoral artery with 5Fr Optitorque used for contralateral shot. The LAD was intervened first. A Runthrough floppy with Microcatheter Finecross, wire escalated to Fielder XT. CTO LAD was successfully crossed and predilated with Sapphire II Pro 2.0 x 15 mm, NSE Alpha 2.5 x 13 mm and NSE Alpha 3.0 x 13 mm balloons. The mid LAD was stented with Resolute Onyx 2.75 x 26 mm and proximal LAD with Xience Alpine 3.0 x 23 mm stent. The stent was further post-dilated with Sapphire II NC 3.5 x 10 mm up to 16 atmospheres.
We intended to treat the OM1 with drug eluting balloon only. We wired down the LCx into OM1, then pre-dilate with a 2.0 x 15 mm balloon at only 6 atmospheres. However, the vessel had dissected. Thus, we changed our strategy to DK-crush 2-stent strategy. OM2 was wired with Sion. We pre-dilated OM2 with NSE Alpha 2.5 x 13 mm. OM1 was stented first with Resolute Onyx 2.5 x 34 mm, then crushed with Sapphire II NC 2.75 x 8 mm. 1st kissing was done. Then we stented OM2 with Resolute Onyx 2.5 x 38 mm. Both stents were post-dilated before final kissing with balloons 2.5 x 10 mm in OM1 and 2.75 x 8 mm into OM2. No POT was performed due to short proximal part of LCx. Before we ended the procedure, we noticed stenosis distal to our previous LAD stent. This was treated with DEB Sequent Please Neo 2.25 x 35 mm balloon with excellent results. Final shots showed no dissections and good TIMI III flow. Right femoral access was closed with Angioseal. 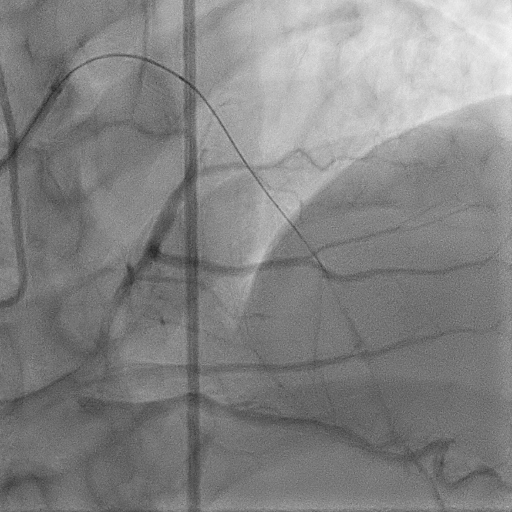 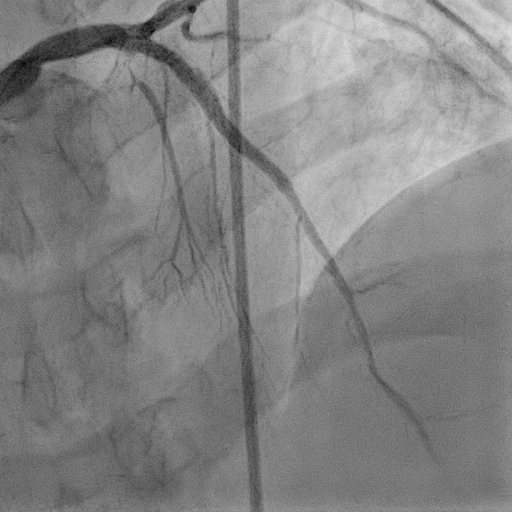 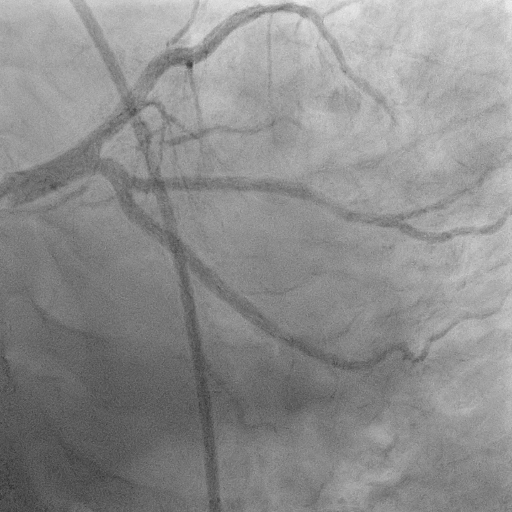 - Case Summary:
Patient was discharged well afterwards. Teaching points are as listed below
1. Dual injection in determining complexity of CTO lesions. - We decided on intervening both LAD and LCx when crossing CTO lesion was determined as not difficult. 2. Improvising from a DEB only strategy to a bifurcation stent strategy in this complex case. 3. Success in delivering two long stents in a bifurcation disease. - no difficulty encountered as both vessels were prepared well. |
|