Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191105_001
| CORONARY - Adjunctive Procedures (thrombectomy, atherectomy, special balloons) | |
| Three Coronary Artery Lesions' Rotational Ablation Come Across Slow Flow and Atrioventricular Block | |
| Qing Yang1, Yifan Guo2 | |
| Beijing Anzhen Hospital, China1, Tianjin medical university General hospital, China2, | |
|
[Clinical Information]
- Patient initials or identifier number:
WJY
-Relevant clinical history and physical exam:
Patient, male, 68 years old, chief complaint: occasional backache for 20 days, aggravate with dyspnea for 1 week.History of hypertension for 10 years, deny the history of diabetes or hemorrhage. Smoking history for 10 years.Physical exam:T: 36.8°, P:61bpm, R:24cpm. A few moist rales have been audible over both lung bases. -Relevant test results prior to catheterization:
ECG: V1-v3 leads' Qs wave ST segment elevation 0.1-0.3mV, v4-v6, I, avL leads' T wave inversion UCG: LVED:53mm IVS:10mm LVEF:33% AO:34mm LVPW:10mm E/A:0.5 TNI: 0.05ng/ml CK-MB: 1.6ng/ml Scr 82umol/L,K+4.2mmol/L,eGFR:86.13ml/min 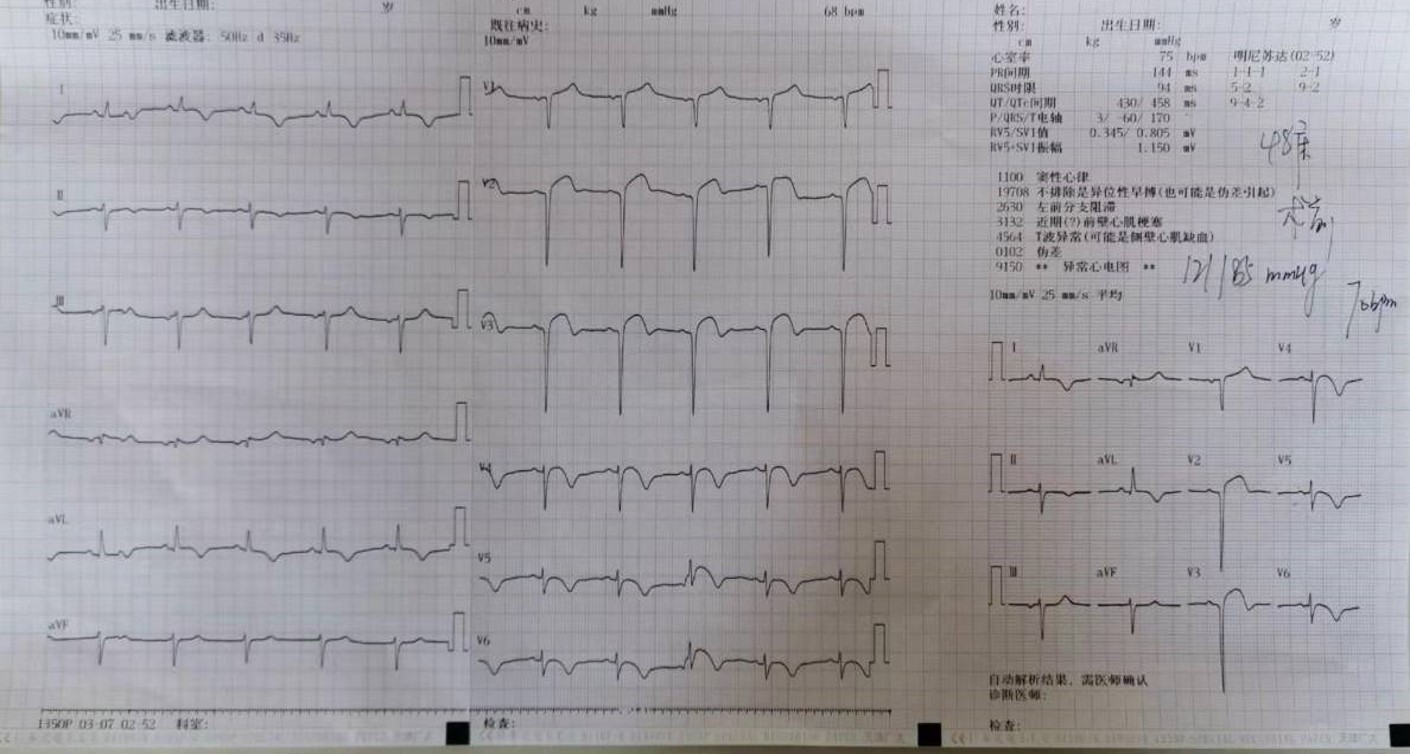 - Relevant catheterization findings:
Left main tube wall irregularLAD stenosis is 99% with severe calcifiedLCX stenosis is 80% with severe calcified
RCA proximal stenosis 70%, middle stenosis 80%,PDA stenosis 70% with severe calcified |
|
|
[Interventional Management]
- Procedural step:
Implantation of IABP pump to maintain hemodynamic stability7F EBU3.5 overhanging the left coronary arteryIVUS probe can’t pass through the stenosis of LADLAD rotational atherectomy by 1.75mm burrPredilation LAD by Quantum2.0×15mmThen we come across the slow flow. We treat slow flow by Injection sodium nitroprusside through microcatheterBail-out alpha 2.5×24mm and Firebird2.75×33mmstentIVUS shows LCX has a 360° Severe calcificationSo we do the LCX rotational atherectomy by1.50mm burrPredilation LCX by Conqueror2.5×15mmBail-out 2.75×24mm stent6F JR4.0 overhanging the RCAIVUS probe can’t pass through the stenosis of RCAThe 2.0×15mm balloon cannot fully predilate RCASo we do the RCA rotational atherectomy by1.50mm burrWhen we do the rotational atherectomy of RCA we come across the second degree of AVBWe treat AVB by Intravenous use of atropine and dopamineAt last we bail-out Premier 2.5×38mm, Premier 3.0×32mm stent in RCA
- Case Summary:
|
|