Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191104_006
| CORONARY - Bifurcation/Left Main Diseases and Intervention | |
| Left Main Quadrifurcation Angioplasty | |
| Sarat Kumar Sahoo1 | |
| Sum Ultimate Medicare, India1, | |
|
[Clinical Information]
- Patient initials or identifier number:
IN
-Relevant clinical history and physical exam:
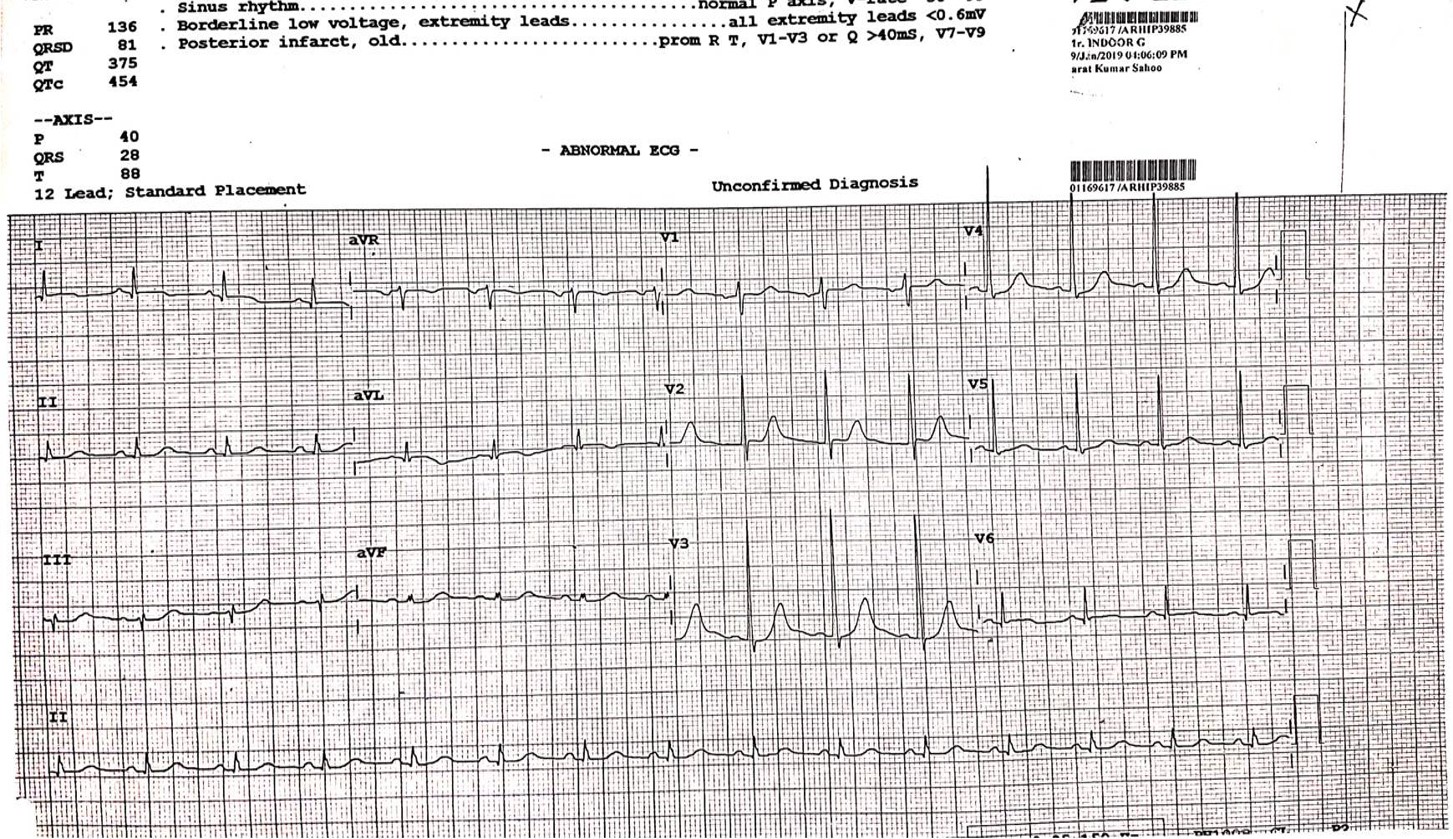
60Yrs/M, On& Off Chest Pain – 2 days, ECG: Posterior Wall STEMI,ECHO: RWMA in LCX,EF-50%
 -Relevant test results prior to catheterization:
•Bifurcation lesions account for 15-20% of all coronary interventions. •Significant LMCA disease is defined as 50% diameter stenosis, corresponding to 75% area stenosis is observed in approximately 5-10% patients who undergo CAG for symptomatic CAD. •Distal LM bifurcation is most commonly involved in upto 80% of cases. •A trifurcation lesion is usually present at distal LM only (LAD,LCX & RI). Can be at LAD-D-S & LCX-OM-PLV. •Anatomically, trifurcation is defined as a close origin of two side branches from the main branch, identified as the distance of both the side branch take-off <3mm and a branch size of atleast2.25mm at baseline angiography or after pre-dilatation. Trifurcation lesion is defined as a diameter stenosis >50% within 5mm from the carina involving the main branch, associated or not with significant disease in either one or both side branches. •Rarely LM can give rise to four branches –LAD,RI,LCX,Accessory RI –Occasionall yearly D from LAD & early OM from LCX can give appearance of quadrifurcation of LM. •Similar to bifurcation left main trifurcation/quadrifurcation (multifurcation), can be classified with the help of modified MEDINA classification. Theoretically 32 anatomical scenarios of left main quadrifurcation involvements are possible. •Left main multifurcation can be –Type-A – Involving LM trunk with extension to one or more of the origin of the branches. –Type-B – Involving origin of one or more of the main branches without extension to LM trunk. 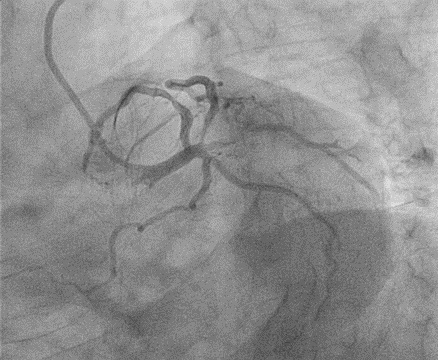 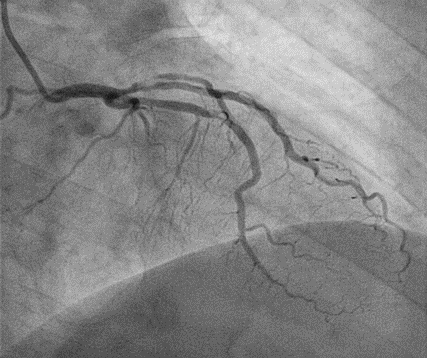 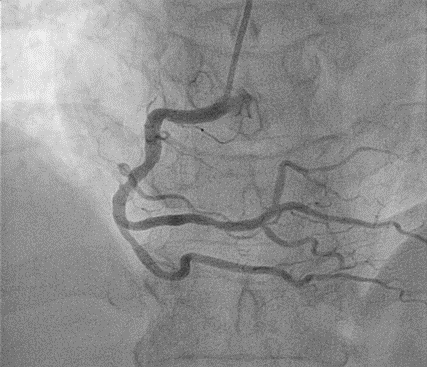 - Relevant catheterization findings:
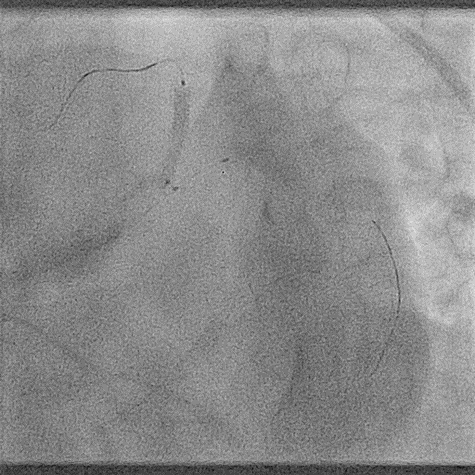
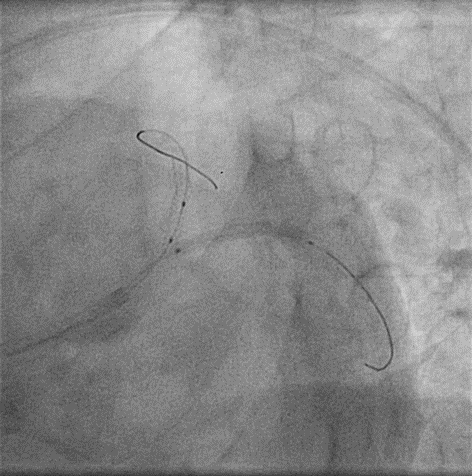
LMCA: Normal, LAD ostioproximal - 50-60% stenosis, Mid – 90% stenosis, ramus intermediate 1 – 70% StenosisRamus intermediate 2 – 90% stenosis, left circumflex – normal, right coronary artery – dominant, mild disease. Plan: Left main quadrifurcation angioplasty
|
|
|
[Interventional Management]
- Procedural step:
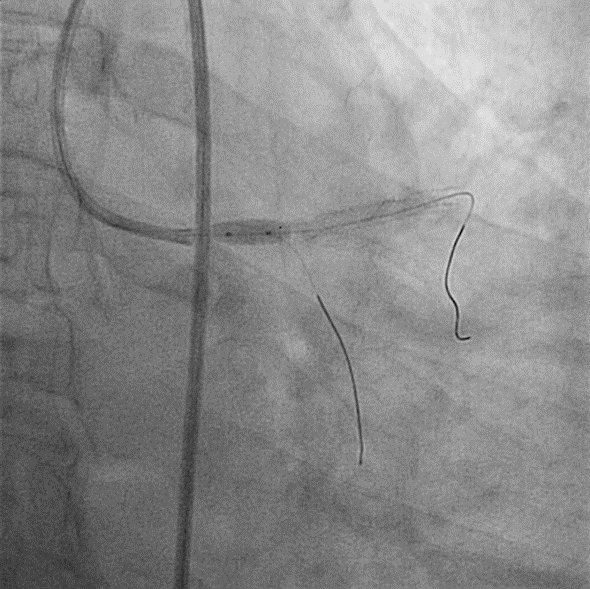
R1&R2- V-Stenting, Angio of after R1 R2 V stenting using 2.75X28 DESs, LM to Mid LAD stenting using 3.5X48 DESFinal kissing balloon dilatation of LAD/LCX, final R1/R2 KBD, final POT. Excellent final result.
   - Case Summary:
Discussion:Treatment option for LM multifurcation is CABG unless it is acute emergency or patient refuses or high risk for surgery.Treatment of LM trifurcation/quadrifurcation percutaneously is complex & challenging, although not impossible.Percutaneous intervention of LM trifurcation/quadrifurcation carries an overall high rate of adverse events mostly driven by a high TLR rate. Type A Lesions and the number of stents placed predicted a higher continued end point of death, non-fatal MI& TLR. Strategy to treat a patient with distal LM stenosis involving trifurcation or quadrifurcation should be individualized. Multiple variables should be considered. Mismatch between proximal distal main vessels. Involvement of daughter vessels number. Size of side branches, Angulation between the branches. Several Techniques can be applicable (V, Y, SKS, T, TAP) for treatingthese lesions, but same techniques like Crush/DK Crush are difficult to plan and have high risk of ISR. Mismatch between LM and Distal Main Branch; Final geometry of the main branch stent; stent will show significant deformations following FKBD with three balloons even though POT & rePOT could be feasible.While treating these lesions, final flow dynamics should be imagined and considered (reduce the turbulence at the LM Multifurcation). Most user friendly approach is provisional approach with bailout TAP, T Stenting of larger side branch; plain balloon dilatation of the smaller side branch ostium and treatment with DEB.
|
|