Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191101_018
| IMAGING AND PHYSIOLOGIC LESION ASSESSMENT - Imaging: Intravascular | |
| Optical Coherence Tomography (OCT) Guided Percutaneous Coronary Intervention of a Patient with Coronary Plaque Rupture | |
| Nay Thu Win1, Ahmad Khairuddin Mohamed Yusof2, Hui Beng Koh3, Mohamed Nazrul Mohamed Nazeeb2, Amin Ariff Nuruddin2 | |
| Royal Free London, United Kingdom1, National Heart Institute, Malaysia2, National Heart Insitute, Malaysia3, | |
|
[Clinical Information]
- Patient initials or identifier number:
RBR
-Relevant clinical history and physical exam:
A 44 years old army officer presented with a complaint of syncope, which resolved spontaneously without residual confusion at emergency department. He also had complaints of headache and chest tightness associated with sweating. He was on intensive army training for 2 days prior to syncope.
-Relevant test results prior to catheterization:
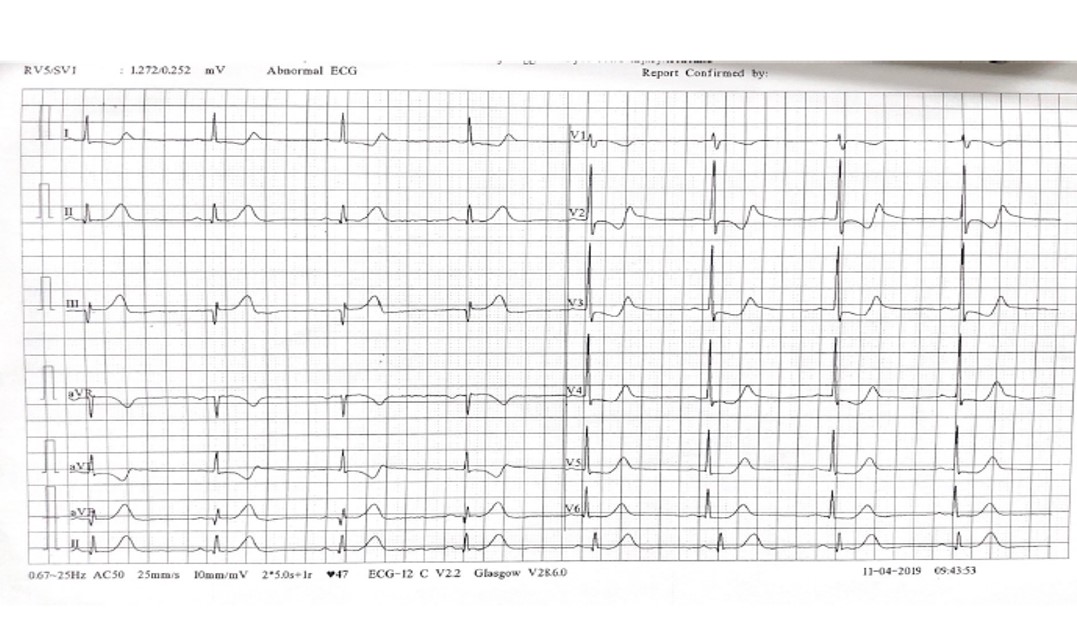
Electrocardiogram showed Q wave in inferior leads with sinus bradycardia. Cardiac enzymes were raised. His renal function, liver function and full blood counts were normal. He was treated as missed inferior myocardial infarct and was transferred to our center for further management.
 - Relevant catheterization findings:
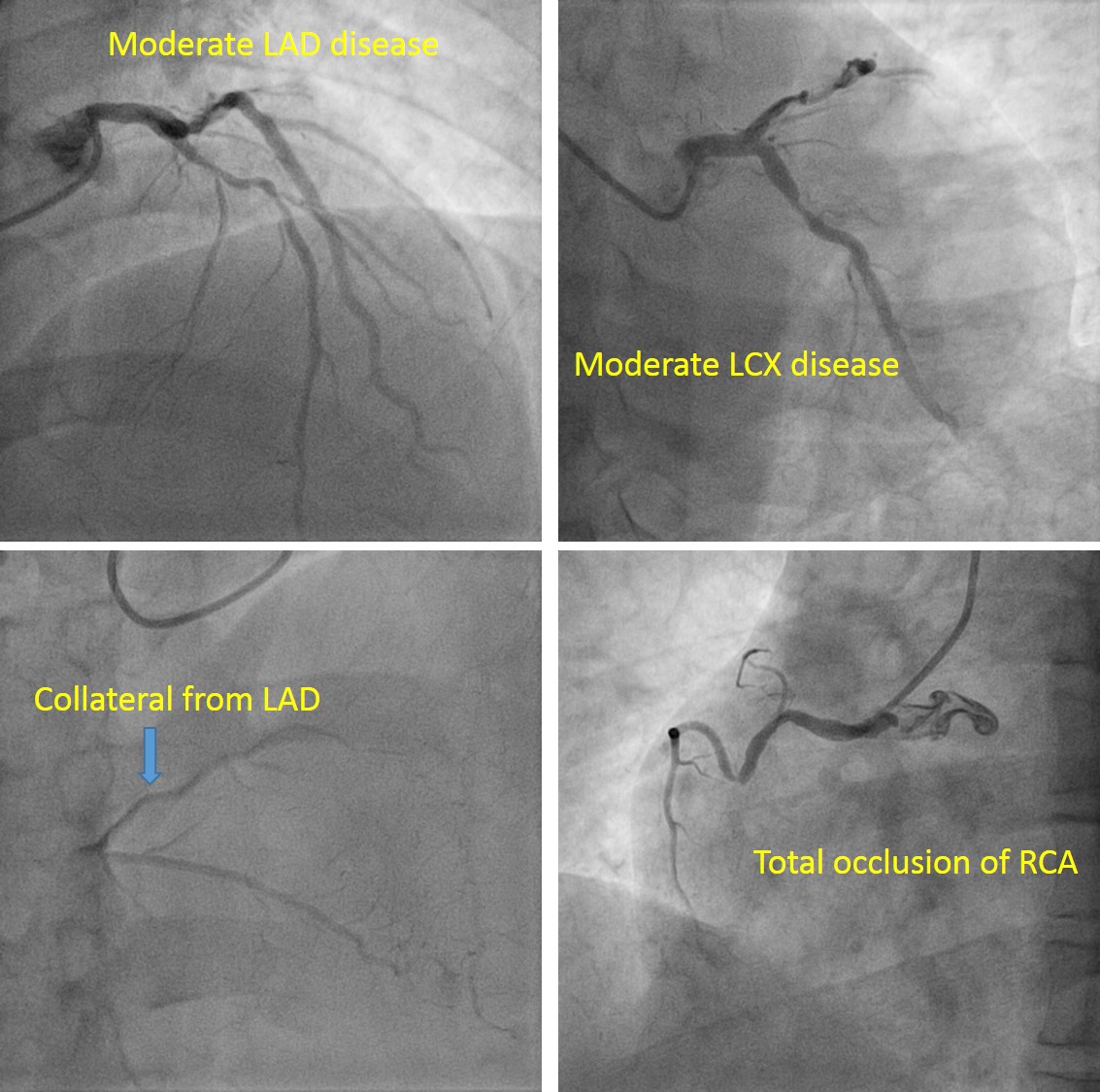
Coronary angiogram showed normal left main stem, moderate proximal left anterior descending, moderate proximal left circumflex disease and total occlusion of right coronary artery with collateral from LAD. Subsequently, we explained the patient regarding the findings and proceeded for coronary angioplasty to RCA.
 |
|
|
[Interventional Management]
- Procedural step:
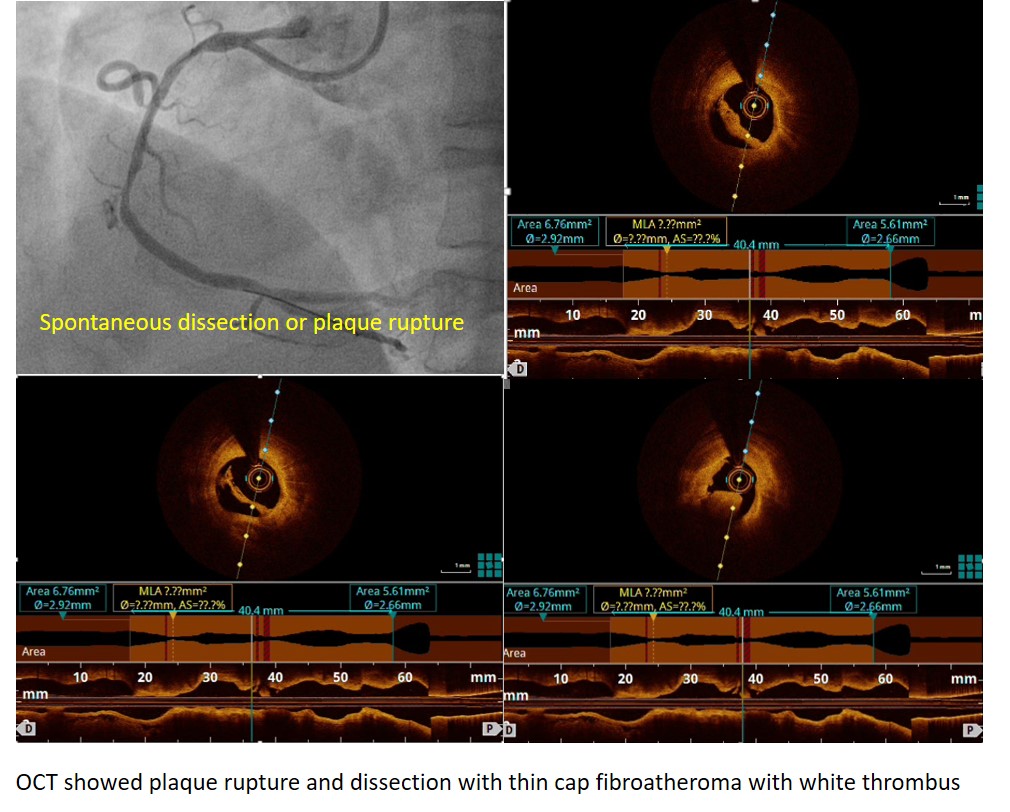
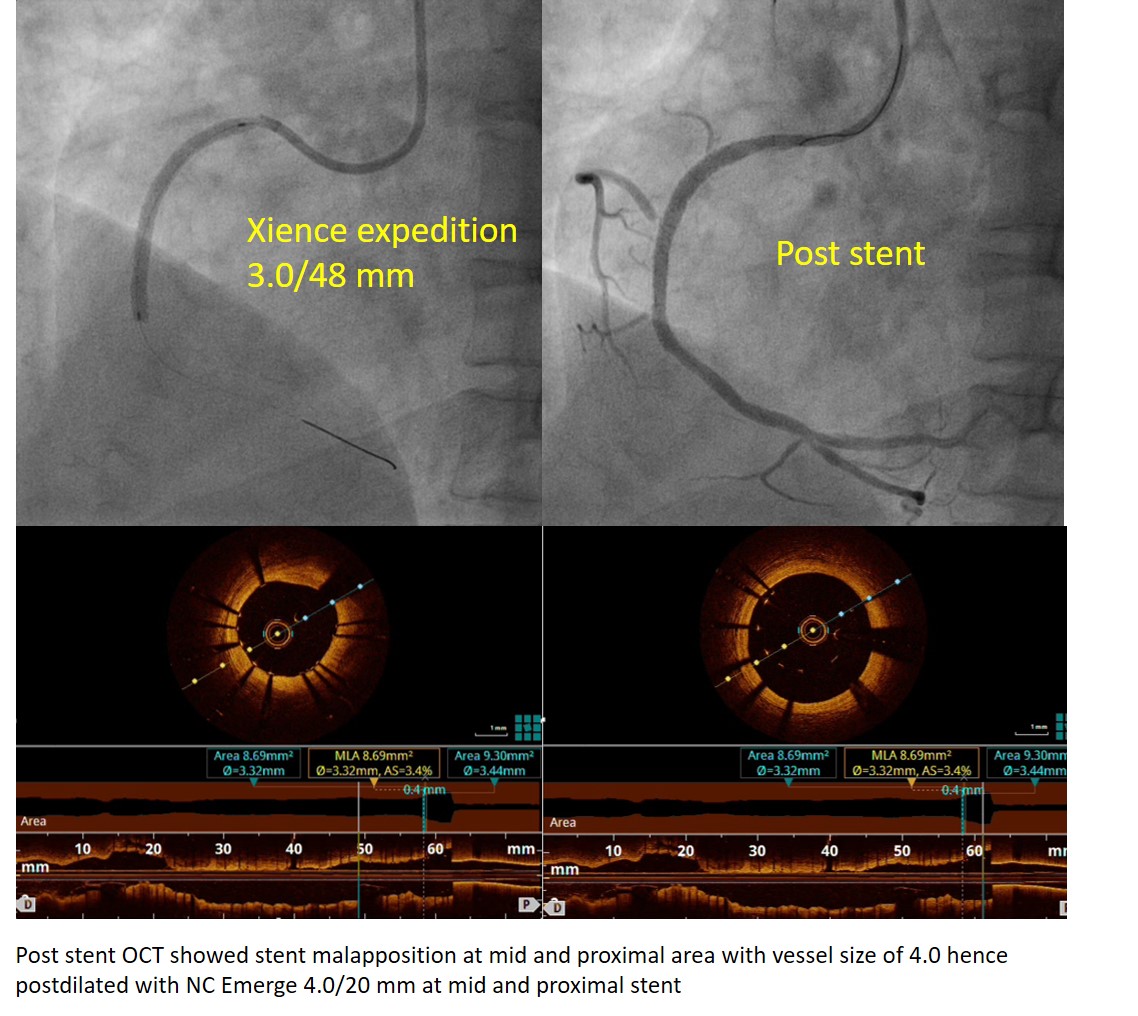
We used guiding catheter short AL1/6F. Runthrough Floppy was used to cross the lesion. We predilated with semi-compliant Sapphire II pro 2.0/15mm to proximal RCA. Despite flow had achieved, we suspected that there was spontaneous coronary artery dissection or coronary plaque rupture in mid RCA. Then, optical coherence tomography was used to understand underlying pathology and assess the lesion characteristic in RCA, which showed plaque rupture and dissection with thin cap fibroatheroma with white thrombus. We predilated again with scoring balloon NC SCOREFLEX 3.0/15 mm at 8 atm. Then stented with Everolimus eluting Xience Expedition 3.0/48 mm to proximal RCA. Post stent OCT showed stent malapposition at mid and proximal area with vessel size of 4.0 hence we postdilated with NC Emerge 4.0/20 mm at mid and proximal stent. Good final result was achieved with TIMI III flow. He was discharged well within 2 days.
  - Case Summary:
The patient developed coronary plaque rupture and acute thrombotic occlusion with underlying atherosclerotic disease, which is most likely precipitated by a strenuous physical activity, presented with syncope. PCI to RCA was done successfully in this patient under OCT guidance. OCT is a useful tool to diagnose underlying pathology, assess lesion characteristic, facilitate lesion preparation, stent sizing as well as confirmation of stent opposition.
|
|