Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191101_012
| ENDOVASCULAR - Peripheral Vascular Disease and Intervention | |
| A Successful Catheter Treatment Case for Traumatic Acute Popliteal Artery Occlusion Using Retrograde Approach via Posterior Tibial Artery | |
| Koichi Yasuda1, Takafumi Koga1, Katsunori Tofuku1, Daisuke Ikeda1 | |
| Ikeda Hospital, Japan1, | |
|
[Clinical Information]
- Patient initials or identifier number:
149668
-Relevant clinical history and physical exam:
A 16-year old man with no prior history was transferred to our hospital following a motorcycle accident. On admission, he was experiencing leg pain. Nobone fracture was found on examination by orthopedic surgeon. A physical examination revealed mild paralysis of the left leg without pallor. The patientwas afebrile, blood pressure was 102/65 mmHg, heart rate 62 beats / minute, and diminished sensation of the entire foot. Left leg pulses were not palpable.
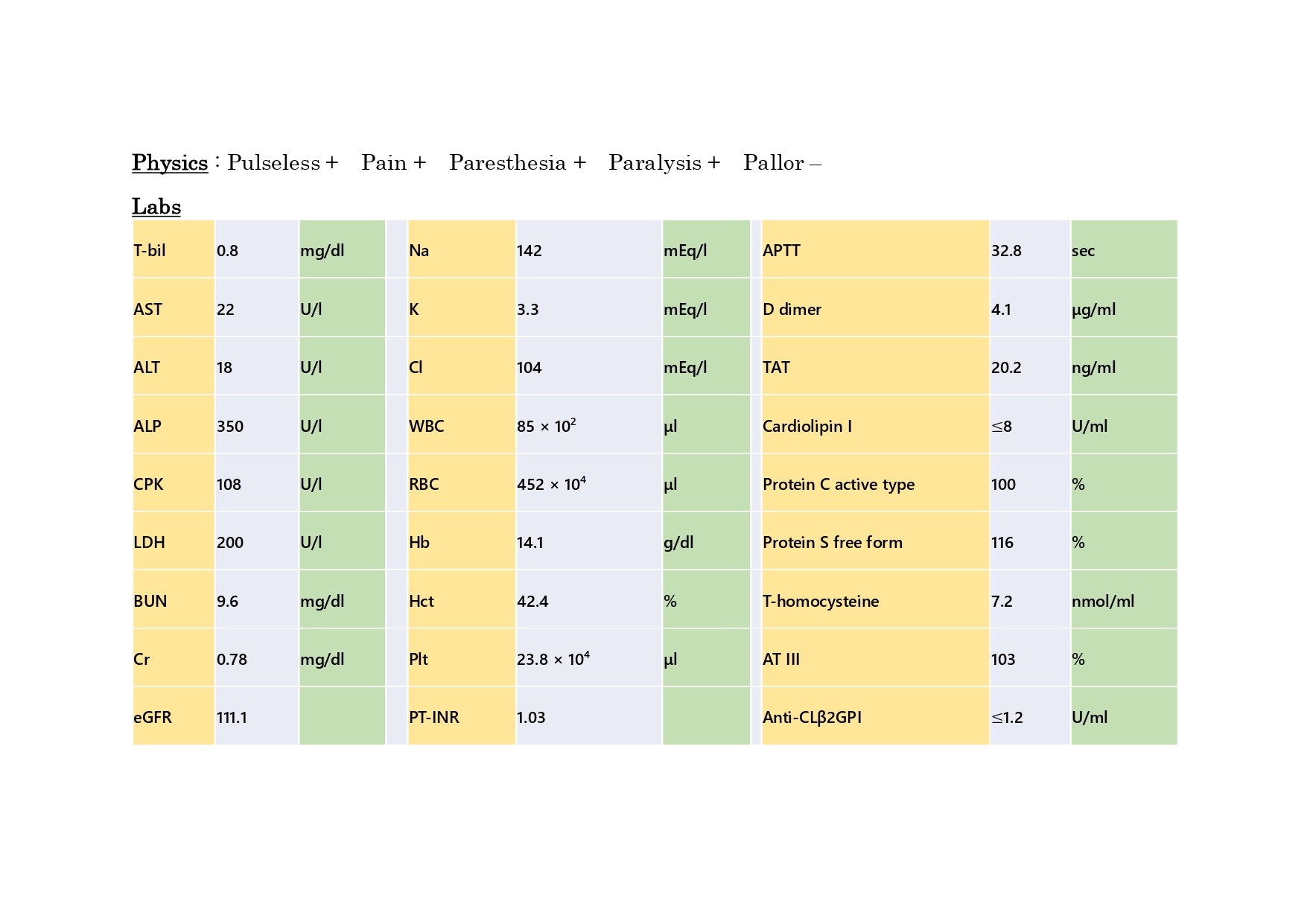 -Relevant test results prior to catheterization:
Before angiography, the result of blood analyses revealed a hematocrit of42.4%. Contrast computed tomography showed fluid in the left posterior femoralmuscle and a contrast defect at the popliteal artery(Video. 1.). Clear contrast extravasation was not found.
- Relevant catheterization findings:
Diagnostic angiography confirmed that the patient had no extravasation. However, the angiography disclosed occlusion of the left popliteal artery(Video. 2.). After a 7Fr.sheath was antegradely inserted into the left common femoral artery, a 0.014floppy wire supported by microcatheter was advanced. The wire did not enter the lesion; therefore, the wire was switched for a 3g wire. However, the wire was advanced inside the subintimal space(Video. 3.).
|
|
|
[Interventional Management]
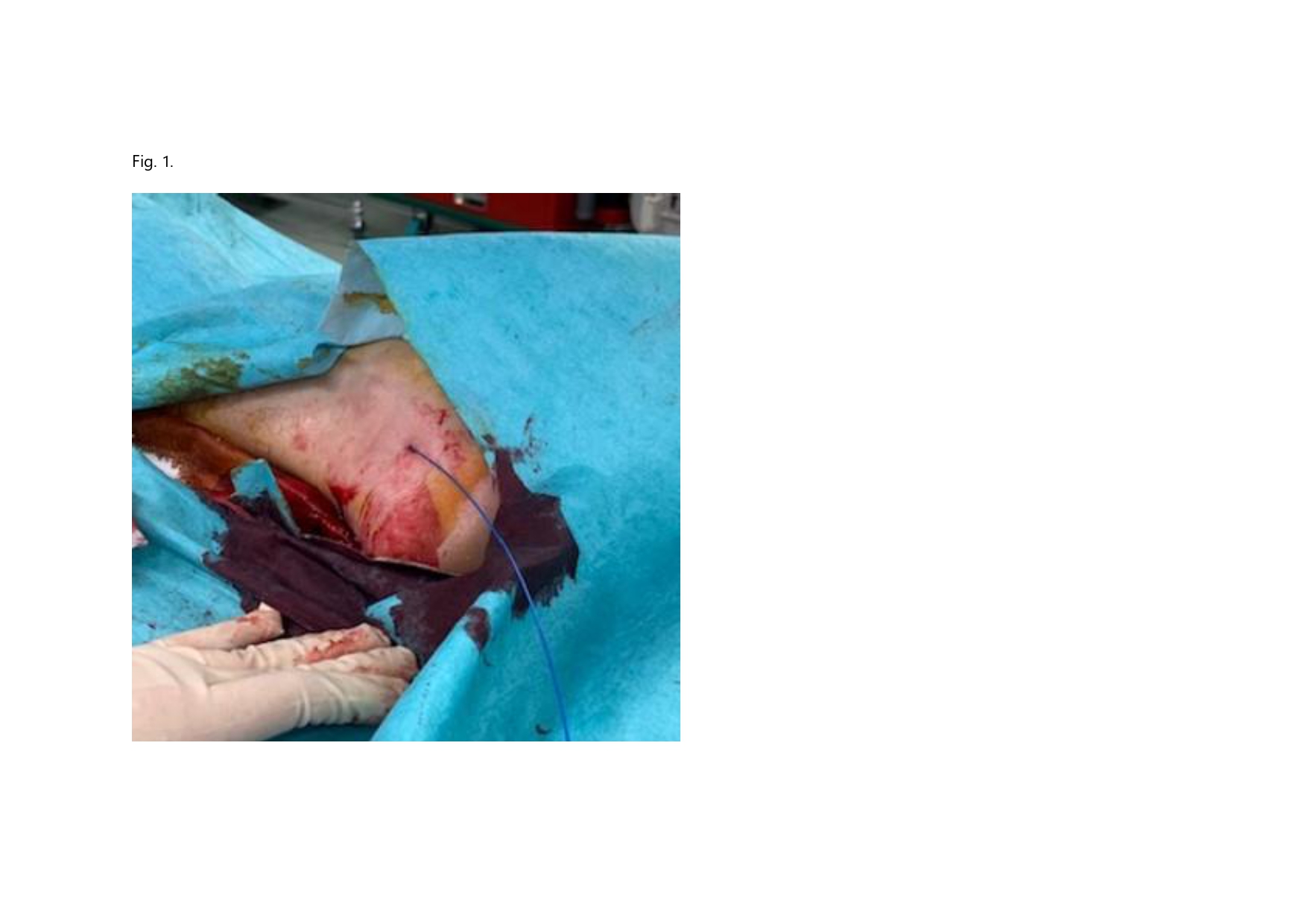
- Procedural step:
We immediately shifted to a retrograde approach(Fig. 1.). The distal posterior tibial artery puncture was easily performed by using vascular ultrasound and a micropuncture kit. The retrograde wire via a sheathless approach passed the lesion easily with no resistance and was externalized. Intravascular ultrasonography demonstrated that the wire was located positioned in the true lumen. After thrombus aspiration, angiography showed partial popliteal artery recanalization. Balloon angioplasty was performed stepwisely with balloons from 2mm to 5mm. Pathologically, the aspirated thrombus was composed of fibrin and blood clots. It was compatible with a fresh thrombus. The final angiogram demonstrated satisfactory flow with minor dissection(Video. 4.). However, 10 days postoperatively, angiography was performed to assess for progression of anemia.Embolization was needed for extravasation at the end of the superior knee artery. After rehabilitation, the patient was released from our hospital without recurrence of an ischemic event 26 days after the operation. Follow-up angiography after 3 months showed complete vessel healing(Video. 5.). From this result, the antiplatelet agent was discontinued.
 - Case Summary:
Blunt vascular injuries of the popliteal artery have a high rate of limb loss. The long patency of popliteal artery stenting is not clear. For young population, intraluminal wiring is essential. In our patient, the antegrade wire migrated into the subintimal space. By using a retrograde approach via the posterior tibial artery, successful endovascular treatment was performed easily and safety. The idea of “leaving nothing behind” after endovascular treatment is a very exiting concept in modern intervention treatment. The retrograde approach is one possible option in such cases.
|
|