Lots of interesting abstracts and cases were submitted for TCTAP & AP VALVES 2020 Virtual. Below are accepted ones after thoroughly reviewed by our official reviewers. Don’t miss the opportunity to explore your knowledge and interact with authors as well as virtual participants by sharing your opinion!
* The E-Science Station is well-optimized for PC.
We highly recommend you use a desktop computer or laptop to browse E-posters.
CASE20191101_010
| STRUCTURAL HEART DISEASE - Congenital Heart Disease (ASD, PDA, PFO, VSD) | |
| Zero Fluoroscopy Transcatheter Closure of Atrial Septal Defect in Adult | |
| Ingrid Maria Pardede1, Sunanto Ng2, Radityo Prakoso | |
| Pelita Harapan University, Indonesia1, Universitas Pelita Harapan, Indonesia2, | |
|
[Clinical Information]
- Patient initials or identifier number:
ANF.RSUS.855617
-Relevant clinical history and physical exam:
We reported a 24-year-old female came with exercise intolerance over the previous 3 months. She had accentuated splitting of second heart sound with grade 3/6 systolic ejection murmur at upper left sternal border.
-Relevant test results prior to catheterization:
Electrocardiogram showed sinus rhythm with right QRS axis and right bundle branch block. Transthoracic echocardiogram revealed right atrial and right ventricular dilatation, D-shaped left ventricular and secundum atrial septal defect (ASD) with left to right shunt.
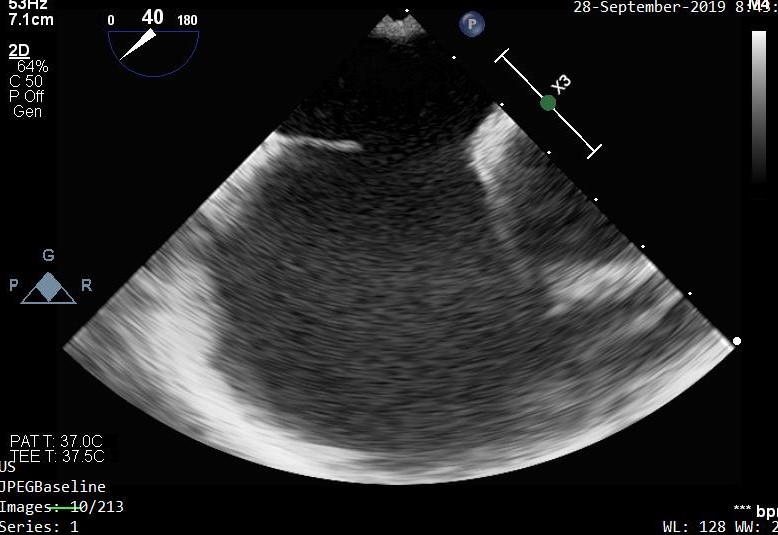
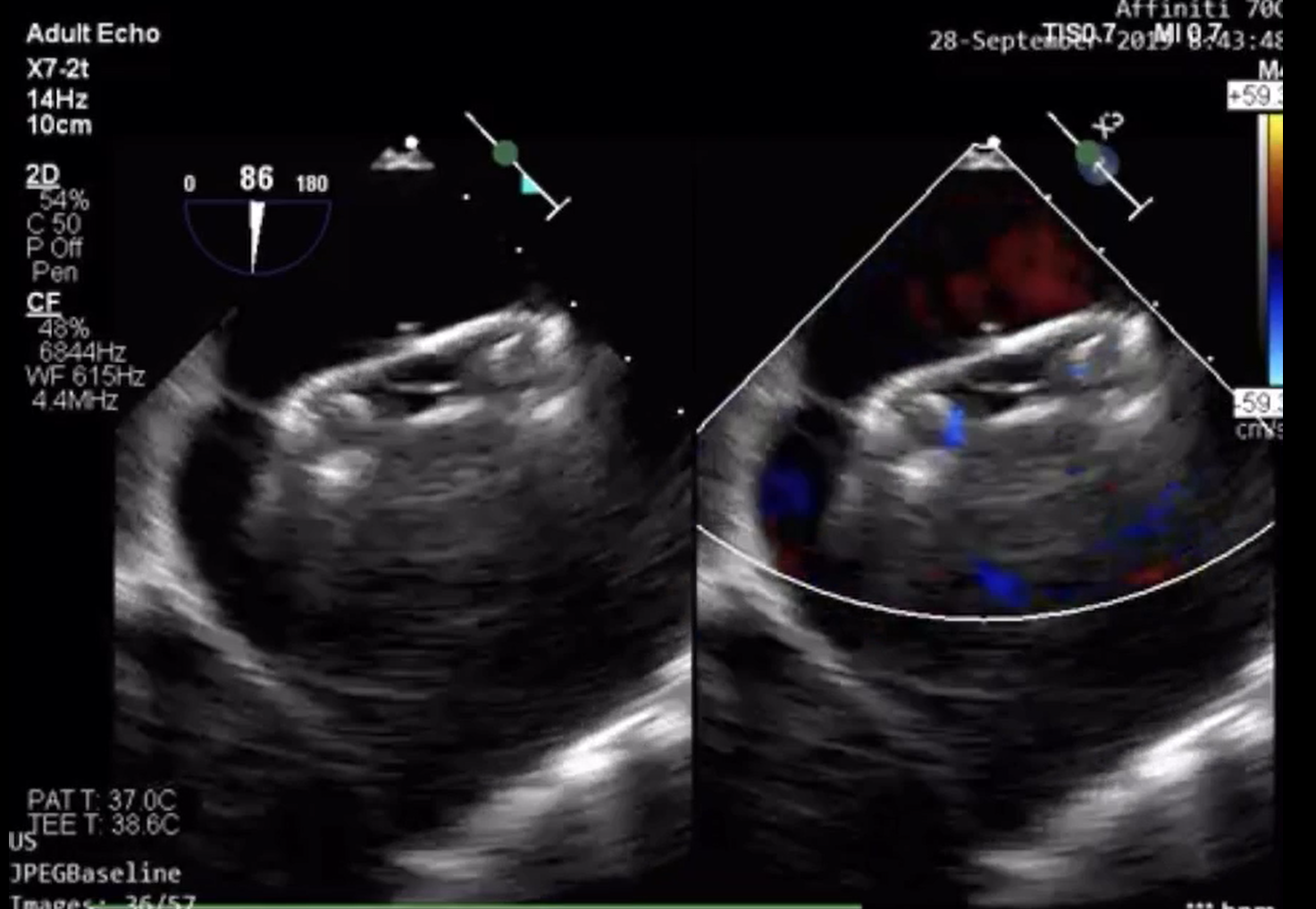
- Relevant catheterization findings:
Transesophageal echocardiogram (TEE) revealed a 19 mm secundum ASD, left to right shunt with complete aortic rim deficiency. The posterior rim was thin and mobile, with adequate length. The superior rim, inferior rim and mitral rim were adequate length. Right heart catheterization has been done prior to current procedure; which revealed high flow-low resistance left-to-right shunt. Mild pulmonary hypertension was documented with pulmonary arterial pressure 64/24 mmHg (mean 37 mmHg).
 |
|
|
[Interventional Management]
- Procedural step:
Transcatheter ASD closure was done under general anesthesia. A 6F side-hole multipurpose (MP) catheter was inserted through right femoral vein. Under the guidance of 2D-TEE, the catheter was advanced to left upper pulmonary vein (LUPV) through the ASD. A 0.035” wire was inserted in LUPV through MP catheter, then the catheter was retrieved. The 12 F delivery sheath was inserted and placed into LUPV. Cera (Lifetech) ASD occluder device no.26 mm was advanced through the delivery sheath into the left atrium under the guidance of TEE. The left disc deployed in the left atrium and pulled back against the atrial septum followed by deployment of right atrial disc. Multiple TEE views evaluation and wiggle test were done. TEE showed optimal position of the atrial occluder device without residual shunt or valve impingement, then the ASD device occlude was released. The ASD closure procedure duration was 22 minutes. No procedure complication occurred.
  - Case Summary:
In conclusion, transcatheter closure of atrial septal defect with transesophageal echocardiography guidance without fluoroscopy is feasible, safe and accurate. Skill in doing zero-fluoroscopy transcatheter intervention should be developed; while it may become essential in patient with contraindication for radiation such as pregnancy.
|
|